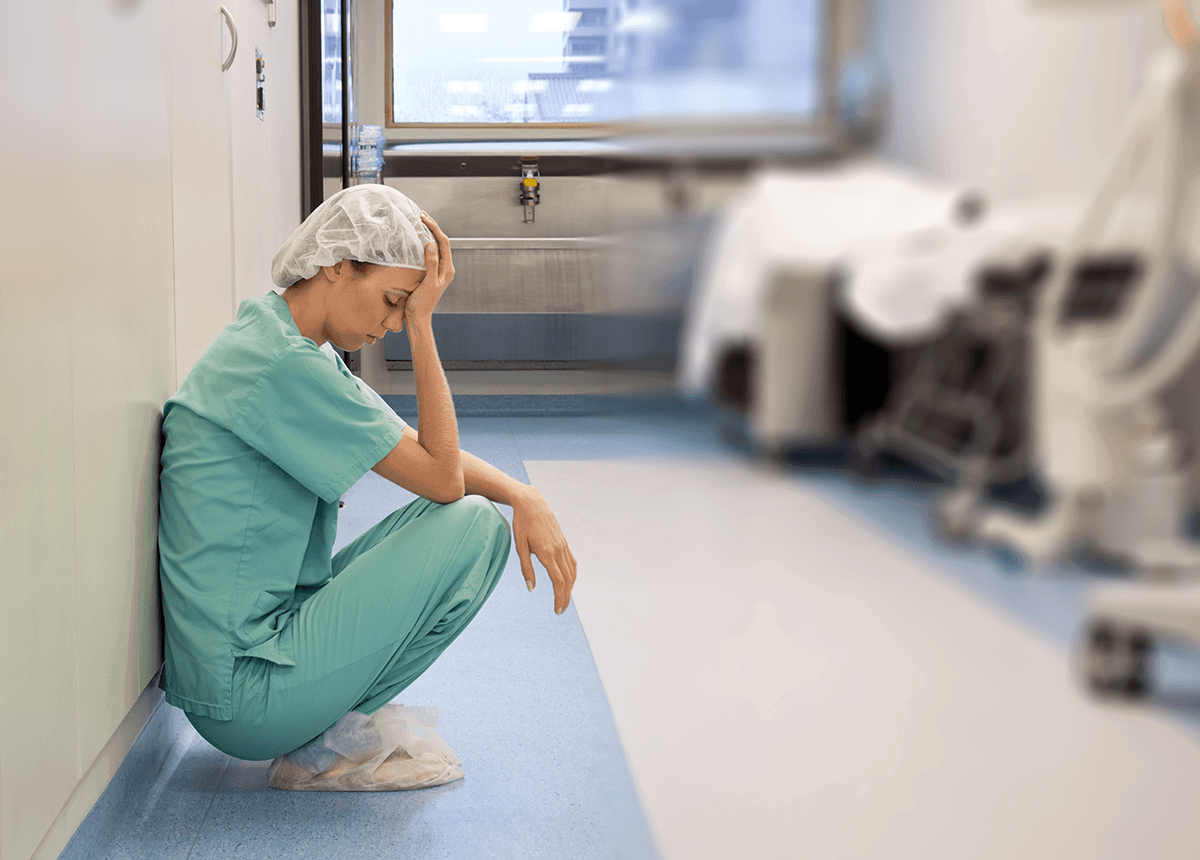
A nurse’s life in the hospital is like the living testament of the saying “expect the unexpected”. One moment everything is under control then suddenly, you’re running around like it’s the end of the world.
Since nursing school, knowing that I fear seeing people dying, I dreaded being assigned in the ER, the ICU, and including the NICU. Fast-forward when I earned my license and was hired to work, I was asked what area I’d like to be assigned to at, with all my heart I answered that I’ll work with patients in a ward.
Four years of nursing school, and as ridiculous as it may sound, I still haven’t overcome my fear of death. It must be that I empathize so much that I always put myself in the shoes of others. I can clearly feel how hard it is losing someone we love so much. The thought and the fact of seeing other people grieve affects me deeply. That is why I choose to work with patients in a ward. Here you get to talk and know the stories of your patients better and most of the time, you get to admit and see them recover— all prep to be discharged. I find this routine of work therapeutic and more relaxing on my part. Seeing death right before my eyes is something that I would never have imagined happening to my patient.
Until this one fateful day where I admitted an 83-year-old patient with pneumonia. His daughters and grandchildren fondly call him “Grandpapa,” but we’ll call him Mr. Smith. From what I’ve learned, he was previously a pastor and lost his wife a year before.
Two days after his admission, Mr. Smith was moved to the ICU. Then for the short time he recovered, he was trammed out and was put in a regular ward under my care for the following days.
Unlike other patients, Mr. Smith is bedridden and in need of total assistance. As his nurse on duty, I did my best to care for this delicate patient. I always do my best to provide the best possible care for my patients but knowing the condition of Mr. Smith was, I know I have to kick my nursing care up a notch. I made my morning rounds with extra care, I checked his vital signs and his LOC, gave his standing order of medications via a nasogastric tube, and made it a point to give my full attention as much as possible when the patient needs something. Shift after shift I can see him recover a bit but sadly he was deteriorating especially during the fourth day.
I was checking the patency of his NGT when I noticed Mr. Smith’s breathing stops for about five seconds of apnea and followed by a series of rapid breaths. I shook my head as I knew that this pattern is a Cheyne-Stokes. Intently, I assessed the gastric residue from his NGT and it was tarry black in color. So I got up and quickly called the attention of the resident on duty to further assess the patient’s status. Although my shift is about to end in an hour (and I’m hungry and tired) it’ll just be heartless to just bust out and leave. I know for myself that your patient is your responsibility.
I relayed my assessments to the ROD and she suspected the patient’s upper gastrointestinal tract is bleeding and gastric lavage with cold water was ordered to help constrict the blood vessels.
During that stressful situation, I was thankful that our head nurse was there to guide and accompany me. The few long breaths I took helped to recompose my nervous self as I started the gastric lavage.
We were able to stabilize Mr. Smith for the next hour when he started declining again. His vitals plummeted down and just in time, the patient’s pulmonologist came and asks to have the emergency cart put on stand by. Another hour has passed and the patient’s O2 saturation was falling fast. I hurriedly called the attention of the RODs and we called out a code. While I was doing my best to participate during the code, I uttered a prayer wanting Mr. Smith to live. Heck, I was praying for a miracle! I wanted to believe that death is inevitable as it is, but can still be avoided.
Unfortunately, this time around it’s not.
The exhausted ROD looked at her wrist and I was downhearted with the next words she said: “Time of death: 8:50 PM.”
Mr. Smith died in front of me. I saw how he never raised his chest again after that last exhale. I saw how his lips and nail beds became pale. Then and there, I started hearing the cries of his daughters. I wanted the time to stop for a while since everything is happening so fast. I wanted to processes everything that happened but I can’t seem to think of anything else during that moment. I kept myself steady and moved away to give the lamenting family time with their Grandpapa. Without me knowing, a single tear came falling from my eyes, then another and then another until I just couldn’t help it. I went out of the room and went straight to the station’s comfort room and there I sat down and burst into tears. And yes, seeing people dying is as bad as I imagine it. More so, it was heartbreaking.
I’ve read in my nursing books about death and dying, we even have a whole lecture day about it. But experiencing it firsthand felt so surreal. During the moment of seeing Mr. Smith passing away, I felt I was very inexperienced and powerless. Everything you’ve learned in nursing school fades while you hear the wails of the patient’s family. You forget what nursing books tell you to do, and you remember the mortality of being a human being and how precious life truly is.
“There I realized that nursing is unfair.”
The whole experience was a hard lesson learned that our profession as a nurse entails seeing and experiencing personally the inevitable cycle of life and death. There I realized that nursing is unfair. Our profession asks us to establish rapport to somebody telling them to beat the odds then suddenly you see them go away. It’s the frequent “trauma” nurses encounter. Another thing I learned from the experience is that you can’t truly control life or death. No matter how advanced medical science is, there are just really things out of your power and it’s sometimes better to let nature take its course. Christine Bell said it best: “Nurses are there when the last breath is taken and nurses are there when the first breath is taken. Although it is more enjoyable to celebrate the birth, it is just as important to comfort in death.”
I haven’t slept well that night. I went home defeated despite my head nurse telling me everything’s going to be okay. I was still thinking of Mr. Smith and how I could have saved him. I could have done more! A week after, Mr. Smith’s daughters came back to the hospital with a box of chocolates for the staff. One of her daughters came to me to personally thank me and gave me a much-needed hug.
In the end, I came to the realization that death is indeed a part of life. And despite everything you’ve done, there are still things that will not go according to what you’ve planned.
Life goes on.






















Leave a Comment