
Nurses play a key role in managing activity intolerance, which affects clients’ ability to perform daily tasks. This care plan guide provides nursing interventions and diagnoses to address reduced tolerance to activity due to surgery, chronic conditions, or prolonged inactivity.
What is Activity Intolerance?
Activity intolerance is a condition in which an individual lacks the physical or mental energy to perform or complete necessary activities.
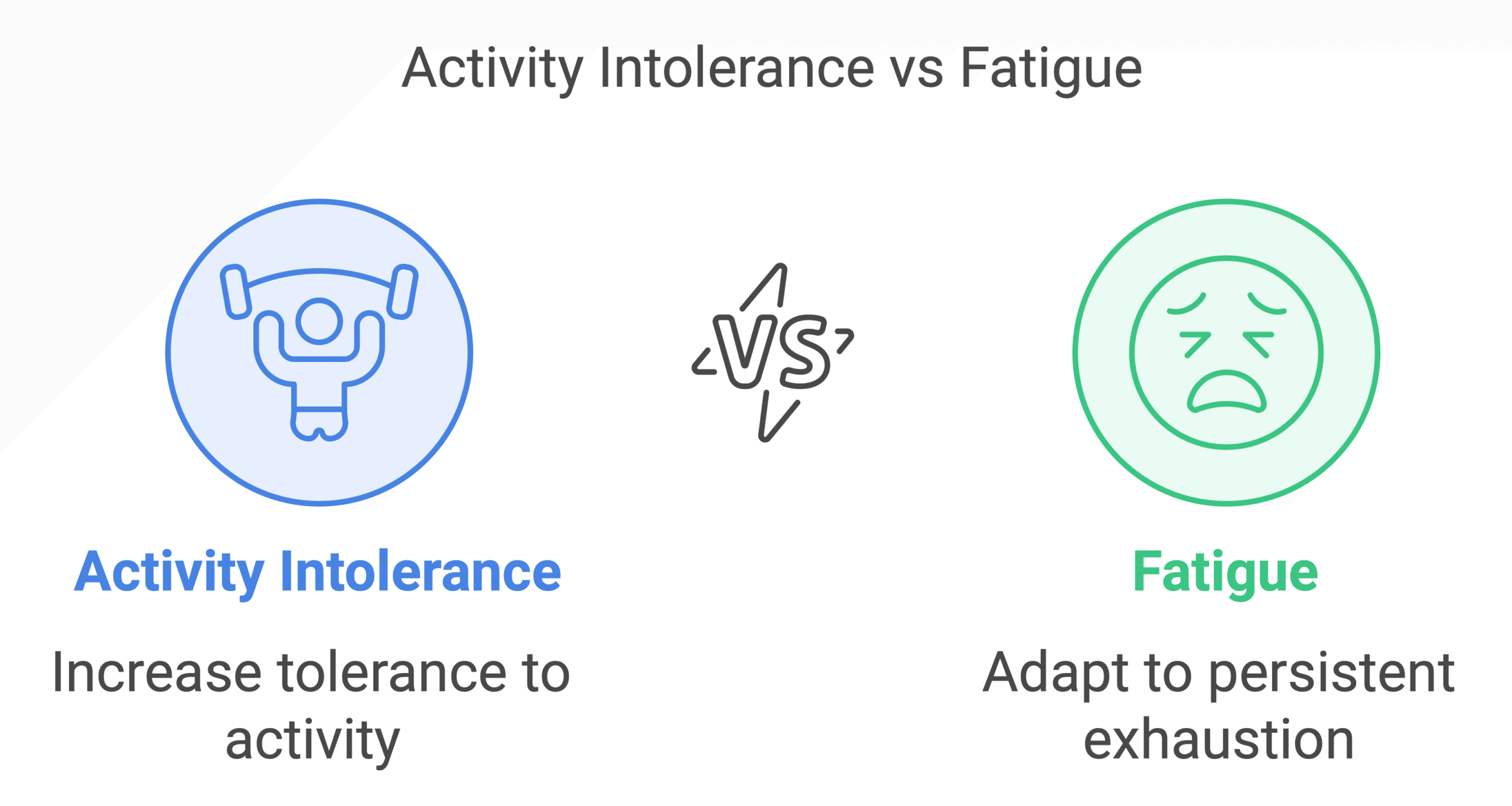
It is different from fatigue, which is a subjective and persistent feeling of exhaustion that can be relieved by rest. The goal of treatment for fatigue is to help the client adapt to the fatigue, while the goal of treatment for activity intolerance is to increase the client’s tolerance to activity.
Causes of intolerance to activity
Activity intolerance or decreased activity tolerance is related to various etiological factors, primarily generalized weakness. Identifying these underlying factors is essential for developing a suitable care plan and implementing targeted interventions to enhance activity tolerance. Specifically, activity intolerance may be related to:
- Cardiovascular conditions. Heart failure, angina, or arrhythmias can lead to reduced cardiac output, impaired blood flow, and compromise in oxygen transport, resulting in activity intolerance.
- Respiratory diseases. Chronic obstructive pulmonary disease (COPD), asthma, or pneumonia can restrict airflow and decrease oxygenation and can cause imbalances between oxygen supply and demand leading to difficulty in performing activities.
- Circulatory diseases such as anemia, hypovolemia, and peripheral arterial diseases can cause an imbalance between oxygen supply and demand.
- Increased metabolic demands such as infection, metabolic disorders, renal diseases, inflammatory diseases, etc.
- Inadequate energy sources due to obesity, malnutrition, or inadequate diet.
- Sedentary lifestyle and physical deconditioning or due to lack of sleep or rest periods.
- Psychological problems such as depression can cause inactivity.
- Surgery or injury due to imposed activity restriction or prolonged bed rest.
- Side effects of medications such as the use of beta-blockers, antihistamines, relaxants, alcohol, and sedatives.
Signs and Symptoms of Activity Intolerance
Recognizing the defining characteristics of activity intolerance is essential for accurate assessment and intervention planning. These characteristics are categorized into subjective data (patient-reported symptoms) and objective data (clinically observed signs), as evidenced by the following:
Subjective Data
- Reports of fatigue or weakness
- Complaints of shortness of breath
- Feeling lightheaded or dizzy
- Descriptions of chest pain or discomfort
- Expressed difficulty completing daily tasks
Objective Data
- Abnormal increase in heart rate during or after activity
- Elevated respiratory rate
- Decreased oxygen saturation levels
- Changes in blood pressure (e.g., hypotension)
- Pale or clammy skin
- Observable shortness of breath or labored breathing
- Inability to complete physical tasks
Nursing Care Plans and Management
This nursing care plan aims to improve the client’s activity tolerance, enhance their functional abilities, and support their overall physical and emotional well-being. It is important to individualize the interventions based on the client’s specific needs and goals, while closely monitoring their response to the interventions and adjusting the care plan as necessary.
Nursing Problem Priorities
The following are the nursing priorities for clients with activity intolerance and generalized weakness:
- Inadequate oxygenation. Clients with activity intolerance experience shortness of breath or reduced oxygen levels during physical exertion. The nurse should monitor oxygen saturation levels and initiate oxygen therapy to improve oxygenation.
- Impaired physical mobility. Activity intolerance causes physical immobility, therefore, the nurse must focus on promoting the client’s ability to perform activities of daily living.
- Risk for falls. Weakness and activity intolerance can increase the client’s risk for falls, leading to injuries. Implementation of fall prevention strategies is essential to keep the client safe.
- Physical deconditioning. Prolonged inactivity can lead to deconditioning of muscles and the cardiovascular system, worsening activity intolerance. Physical activity and exercise programs are vital to avoid this problem.
Nursing Assessment
Ongoing assessment is essential in order to identify potential problems that may have led to decreased tolerance to physical activity and generalized weakness as well as identify any issues that may arise during nursing care. Identifying and addressing these symptoms is crucial for managing a decrease in tolerance to activity and developing appropriate nursing interventions to improve functional abilities and quality of life.
Assess for the following subjective and objective data:
- Generalized weakness. A feeling of overall reduced strength or lack of energy makes it difficult to perform activities.
- Shortness of breath. Breathlessness or difficulty breathing during physical exertion or even mild activities.
- Rapid heart rate. An abnormally fast heartbeat or palpitations occur with minimal activity or exertion.
- Excessive fatigue. A persistent feeling of tiredness, exhaustion, or lack of energy hinders the ability to engage in activities.
- Muscle pain or discomfort. Unexplained muscle aches, soreness, or discomfort during or after activities.
- Dizziness or lightheadedness. Feeling unsteady, dizzy, or faint during or after physical exertion.
- Verbal reports of weakness. Inability to perform or endure desired activities.
- Sudden facial pallor. This refers to the paleness of the skin due to reduced blood flow to the peripheral tissues, including the skin.
Nursing Diagnosis
After thorough assessment, nursing diagnoses are formulated to address the challenges of decreased tolerance to activity, guided by the nurse’s clinical judgment and understanding of the patient’s unique condition. While nursing diagnoses help organize care, their use may vary across clinical settings. Ultimately, the nurse’s expertise and judgment shape the care plan to prioritize each patient’s needs. Here are examples of nursing diagnoses that may be useful for common concerns associated with activity intolerance:
- Activity Intolerance related to decreased energy levels and lack of physical conditioning as evidenced by verbal reports of fatigue, inability to complete basic activities of daily living, and increased pulse rate after minimal exertion.
- Activity Intolerance related to inadequate energy reserves as evidenced by complaints of weakness, dyspnea with activity, and observed difficulty in maintaining physical activity.
- Activity Intolerance related to sedentary lifestyle as evidenced by decreased muscle strength, fatigue during simple tasks, and reliance on assistance for ambulation.
- Activity Intolerance related to impaired physical endurance as evidenced by shortness of breath with mild activity, reports of needing frequent rest periods, and observable exhaustion following minimal exertion.
- Activity Intolerance related to poor nutritional intake as evidenced by muscle weakness, patient reports of fatigue, and inability to sustain activity without rest.
- Activity Intolerance related to limited mobility and physical deconditioning as evidenced by complaints of generalized weakness, increased respiratory rate post-activity, and inability to perform self-care activities independently.
Nursing Goals
The following are the common nursing care planning goals and expected outcomes for clients with decreased tolerance to activity.
- The client will identify the factors that aggravate decreased tolerance to activity.
- The client will identify methods and techniques to reduce activity intolerance.
- The client will demonstrate methods of controlled breathing techniques to conserve energy.
- The client will describe adaptive techniques to perform activities of daily living.
- The client will participate in necessary and desired activities.
- The client will report a measurable, progressive increase in activity tolerance.
- The client will display laboratory values within an acceptable range.
Nursing Interventions and Actions
The following are the therapeutic nursing interventions for clients with activity intolerance:
1. Assessment of Physical Ability and Mobility
By determining the appropriate activity level for a client, the nurse can predict whether the client has the strength and endurance to participate in activities requiring similar expenditures of energy.
Assess the client’s level of activity tolerance and difficulties in mobility
Assess the physical activity level and mobility of the client.
This is to provide baseline information for formulating nursing goals and to help guide nursing interventions. Assessment to monitor the client’s response to activity should include the following steps:
- Take the resting pulse, blood pressure, and respiration.
- Consider the rate, rhythm, and quality of the pulse.
- If the signs are normal, have the client perform the activity.
- Obtain the vital signs immediately after activity
- Have the client rest for three minutes and then take the vital signs again.
Discontinue the activity if the client responds with:
- Chest pain, vertigo, and/or dizziness
- Decreased pulse rate, systemic blood pressure, respiratory response
Reduce the duration and intensity of the activity if:
- The pulse takes longer than three minutes to return to within six to seven beats of the resting pulse.
- RR increase is excessive after the activity.
Investigate the client’s perception of the causes of activity intolerance.
Causative factors may be temporary or permanent as well as physical or psychological. Determining the cause can help guide the nurse during the nursing intervention. Activity intolerance can be influenced by disease process factors, energy levels, age and development, circulatory status, neurological factors, and psychological factors (Andriani et al., 2022). Self-perception can be related to the cognitive and emotional processes that people use to formulate their beliefs and feelings about themselves.
Determine the client’s level of activity intolerance.
This is to provide a baseline for comparison and track the client’s progress. Changes in the client’s activity tolerance are often gradual and may go unnoticed. The nurse determines if there are recent changes by comparing the client’s current activity levels with that performed in the past 6 to 12 months.
| Level | Description |
|---|---|
| Level I | Walk at a regular pace on level ground indefinitely; climb one flight or more but experience shortness of breath beyond normal. |
| Level II | Walk one city block or 500 ft on level ground; climb one flight of stairs slowly without stopping. |
| Level III | Walk no more than 50 ft on level ground without stopping; unable to climb one flight of stairs without stopping. |
| Level IV | Experience dyspnea and fatigue at rest. |
Assess the need for ambulation aids (e.g., cane, walker) for ADLs.
Assistive devices enhance the mobility of the client by helping them overcome limitations. Additionally, the nurse assesses the client’s ability to use various assistive devices that promote mobility. If the client cannot ambulate without assistance, the nurse assesses the client’s ability to balance, transfer, and use assistive devices.
Assess the client’s baseline cardiopulmonary status (e.g., heart rate, orthostatic BP) before initiating activity.
In normal adults, HR should not increase more than 20 to 30 beats/min above resting with routine activities. Older adults are more susceptible to orthostatic drops in BP with position changes. Dramatic changes in the client’s cardiopulmonary status result from an imbalance of oxygen supply and demand. Specifically, assess for any increase in pulse rate, marked fall in blood pressure, dizziness, light-headedness, and dimming of vision when the client moves from a supine to a vertical posture.
Determine the client’s level of functional ability.
Functional ability is an individual’s ability to perform ADLs and instrumental activities of daily living. One of the most frequently used tools to assess the client’s level of independence is the Functional Independence Measure (FIM). The FIM is a minimum data set, measuring 18 self-care items including bathing, grooming, dressing, toileting, bladder management, and bowel management.
Assess the client’s strength and ability to move.
Before the client changes their position or attempts to ambulate, the nurse must assess the client’s strength and ability to move first. Assessment of upper extremity strength is especially important for clients who use ambulation aids, such as walkers and crutches.
Assess the client’s degree of comfort.
Some clients who have pain may not want to move and may require an analgesic before they are moved. Previous experimental research has shown that pain catastrophizing is associated with communicative pain behaviors and activity intolerance. Investigations have also shown that fear of movement or re-injury is associated with activity intolerance (Thibault et al., 2008).
Determine the client’s cognitive abilities and limitations.
Mental alertness and the ability to follow directions are necessary for the client to perform daily activities. Check whether the client is receiving medications that hinder the ability to walk safely. Narcotics, sedatives, tranquilizers, and some antihistamines cause drowsiness, dizziness, weakness, and orthostatic hypotension.
Assess the client’s coordination and balance.
Determine the client’s abilities to hold the body erect, bear weight and keep balance in a standing position on both legs or only one, to take steps, and to push off from a chair or bed. The client is instructed to walk across the room, if possible, while the nurse observes posture and gait. The Romberg test is a screening test for balance that can be done with the client seated or standing.
Assess the etiological factors and effects of activity intolerance
Assess the client’s nutritional status.
Adequate energy reserves are needed during activity. Nutritional deficiencies can lead to weakness, fatigue, and decreased endurance, making it more difficult for a person to tolerate activity. Assessment of a client’s nutritional status can help identify deficiencies that may be affecting their decreased activity tolerance. The nurse should obtain the following information:
- The client’s current height and weight
- The client’s dietary patterns on a typical day and any food preferences
- Eating habits
- Who shops for groceries and prepares meals
Observe and monitor the client’s sleep pattern and the amount of sleep achieved over the past few days.
Sleep deprivation and difficulties during sleep can affect the activity level of the client – these need to be addressed before successful activity progression can be achieved. Clues to worsening cardiac disease, especially heart failure, can be revealed by sleep-related events. Clients with worsening HF often experience orthopnea, the indeed to sit upright or stand to avoid feeling short of breath. The client may report that they need to sleep upright in a chair or add extra pillows to their bed.
Determine the client’s daily routine and over-the-counter medication.
Fatigue can limit the client’s ability to perform needed activities. It can also be a medication side effect. Pay attention to the client’s use of beta-blockers, calcium channel blockers, tranquilizers, antihistamines, relaxants, alcohol, and sedatives. The nurse should ask about the following information to ensure that the client is safely and effectively taking these medications:
- Names and doses of medications
- Purpose of each medication
- Timing of medication intake
- Any skipped doses of these medications
Assess emotional response to limitations in physical activity.
Depression over the inability to perform activities can be a source of stress and frustration. Clients with a diagnosis of myocardial infarction and depression have an increased risk of rehospitalization, death, more frequent angina, more physical limitations, and poorer quality of life compared with clients without depression.
Use portable pulse oximetry to assess for oxygen desaturation during activity.
This may determine the use of supplemental oxygen to help compensate for the increased oxygen demands during physical activity. Normal oxygen saturation values are more than 95%. Values less than 90% indicate that the tissues are not receiving enough oxygen, in which case further evaluation is required.
Assess the level of dyspnea during or after an activity.
In chronic lung diseases, dyspnea is first reported during physical activity and generally reflects an increased neural drive to the respiratory muscles overburdened by increased intrinsic mechanical loading. Dyspnea can be assessed based on how it affects functional ability, employment, quality of life, or health status (Hanania & O’Donnell, 2019).
Utilize the Borg Scale for dyspnea and fatigue.
A real-time evaluation of symptoms only answers the question of how hard the dyspnea or fatigue was experienced during the test. The Borg sale is a very simple numerical list used to assess the Rating of Perceived Exertion. Clients are asked to rate exertion during activity by combining all sensations of physical stress and fatigue. They are told to ignore other factors such as shortness of breath or leg fatigue by trying to focus on the sensations of exertion.
Assist the client during the cardiopulmonary exercise testing (CPET).
The level of intolerance and exercise capacity is clinically determined by the CPEt test, which is a non-invasive technique to evaluate the integrative functions of the cardiovascular, respiratory, hematopoietic, metabolic, and neuropsychological systems during maximal exercise. This test is considered a gold standard to assess exercise capacity and objectively determine intolerance.
Monitor the client’s hemoglobin levels.
A client who has become gradually anemic, with hemoglobin levels between 9 and 11 g/dL, usually has fewer or no symptoms other than slight tachycardia on exertion and possibly fatigue. Clients who are very active or who have significant demands on their lives are more likely to have symptoms, and those symptoms are more likely to be pronounced than in more sedentary people.
2. Improving Physical Mobility and Activity Level
Before the client undertakes a change in position or attempts to ambulate, it is essential for the nurse to assess the client’s strength and ability to move. Range of motion exercises and specific therapeutic exercises may be included in the implementation of interventions.
Improving tolerance to activity
Establish guidelines and goals of activity with both the client and significant others (SO).
Motivation and cooperation are enhanced if the client participates in goal setting. To enhance adherence, the nurse should assist the client to develop goals to incorporate the therapeutic plan into everyday activities rather than merely giving the client a list of instructions.
Provide emotional support and a positive attitude regarding abilities.
The client may be fearful of overexertion and potential damage to the heart. Appropriate supervision during early efforts can enhance confidence. Being diagnosed with conditions that affect activity tolerance, such as leukemia, COPD, or heart failure, can be extremely frightening. In many instances, the need to begin treatment is emergent, and the client has little time to process the fact that they have the illness before making decisions about therapy. Providing emotional support and discussing the uncertain future is crucial.
Have the client perform the activity more slowly, in a longer time with more rest or pauses, or with assistance if necessary.
This helps in increasing the tolerance for the activity. At a minimum, the client should be encouraged to sit up in a chair while awake rather than staying in bed; even this simple activity can improve the client’s tidal volume and enhance circulation.
Gradually increase activity with active range-of-motion exercises in bed, increasing to sitting and then standing.
Gradual progression of the activity prevents overexertion. Duration and frequency should be increased first before intensity. Range of motion involves moving a joint through its full range in all appropriate planes. These exercises are planned for individual clients to accommodate the wide variation in the degrees of motion that people with varying body builds and age groups can attain. These activities can include:
- Range-of-motion (ROM) exercises in bed, gradually increasing duration and frequency (then intensity) to sitting and then standing.
- Deep-breathing exercises three or more times daily.
- Sitting up in a chair for 30 minutes three times daily.
- Walking in the room for one to two minutes three times a day.
- Walking down the hall 20 feet or walking through the house, then slowly progressing walking outside the house, saving energy for the return trip
Dangle the legs from the bedside for 10 to 15 minutes.
This helps prevent orthostatic hypotension. Prolonged immobility can impair the body’s ability to constrict blood vessels, leading to blood pooling in the legs and a drop in central blood pressure, which reduces adequate blood flow and perfusion.
Refrain from performing nonessential activities or procedures.
The client with limited activity tolerance needs to prioritize important tasks first. The nurse may assist the client to prioritize activities and to establish a balance between activity and rest that is acceptable to the client. The client will still need to maintain some physical activity and exercise to prevent deconditioning that results from inactivity.
Assist with ADLs while avoiding client dependency.
Assisting the client with ADLs allows conservation of energy. Carefully balance the provision of assistance; facilitating progressive endurance will ultimately enhance the client’s activity tolerance and self-esteem. The nurse must aid the client to identify the safe limits of independent activity; knowing when to ask for assistance is particularly important.
Provide bedside commode as indicated.
The use of a commode requires less energy expenditure than using a bedpan or ambulating to the bathroom. Additionally, the use of a commode involves assuming a normal anatomic position for voiding, which facilitates urination in clients with urinary retention due to prolonged immobility.
Encourage physical activity consistent with the client’s energy levels.
This helps promote a sense of autonomy while being realistic about capabilities. Physical activity is proven to improve lung function, muscle strength, and other positive impacts for a client with COPD. The most effective intervention found in studies is the upper extremity resistance exercise intervention, which has profound effects on aerobic capacity, muscle strength, and quality of life (Shalahuddin et al., 2022).
Instruct the client to plan activities for times when they have the most energy.
Activities should be planned ahead to coincide with the patient’s peak energy level. If the goal is too low, negotiate. For example, bathing, dressing, grooming, and fixing breakfast in the morning before work can be too much for the client. Instead, the client may shower at night before going to bed. Non-perishable breakfast items can be set out the night before to lessen the client’s workload during the day (Buzaid et al., 2013).
Encourage verbalization of feelings regarding limitations. Provide a positive atmosphere.
Verbalization of feelings can help the client to cope and minimizes frustration. Mental or affective disorders such as depression or chronic stress may affect the client’s desire to move. Acknowledge the client’s feelings about activity intolerance as this can be both physically and emotionally difficult. This can foster a more empathetic and compassionate relationship between the nurse and the client.
Encourage active ROM exercises. Encourage the client to participate in planning activities that gradually build endurance.
Exercise maintains muscle strength, joint ROM, and exercise tolerance. Physical inactive clients need to improve functional capacity through repetitive exercises over a long period of time. Strength training is valuable in enhancing the endurance of many ADLs. when performed correctly, exercise assists in maintaining and building muscle strength, maintaining joint function, preventing deformity, stimulating circulation, developing endurance, and promoting relaxation.
Provide the client with the adaptive equipment needed for completing ADLs.
Appropriate aids will enable the client to achieve optimal independence for self-care and reduce energy consumption during activity. The devices may include built-up handles on toothbrushes and razors; long curved handles on mirrors or shoe horns; suction cups to hold items in place; shower chairs; raised toilet seats; and universal cuffs to grip self-care items.
Evaluate the need for additional help at home.
Coordinated efforts help the client conserve energy more effectively. If a caregiver is needed, the client and family should learn how to manage them. The nurse should assist the client in accepting self-care dependency while promoting independence in areas like social interaction to support a positive self-concept.
For clients with pulmonary insufficiency
Encourage conscious-controlled breathing techniques (e.g., pursed-lip breathing and diaphragmatic breathing) during increased activity and times of emotional or physical stress.
This helps in performing efficient breathing by maximizing the expansion of the lungs. Techniques can include the following:
Pursed-lip breathing
The goal of pursed-lip breathing is to prolong exhalation and increase airway pressure during expiration, thus reducing the amount of trapped air and the amount of airway resistance.
- Have the client breathe in through the nose while slowly counting to three.
- Allow the client to exhale slowly and evenly against pursed lips.
- The client counts to seven slowly while prolonging expiration through pursed lips.
Diaphragmatic breathing or abdominal breathing
The goal of diaphragmatic breathing is to use and strengthen the diaphragm during breathing.
- Have the client sit comfortably with knees bent and shoulders, head, and neck relaxed.
- The client should place one hand on the upper chest and the other just below the rib cage to allow the palpation of the movement of the diaphragm during breathing.
- The client breathes in slowly through the nose so that the stomach moves out against their hand. The hand on the chest should remain as still as possible.
- Tighten the stomach muscles, letting them fall inward during exhalation through pursed-lip.
- These steps are repeated for one minute, then followed by a rest period of two minutes.
Pace the client’s activity and rest periods.
Clients with COPD have decreased exercise tolerance during specific periods of the day, especially in the morning on arising, because bronchial secretions have collected in the lungs during the night. Activities that require the arms to be supported above the level of the thorax may produce fatigue or respiratory distress but may be tolerated better after the client has been up and moving around for an hour or more.
Instruct the client to coordinate breathing exercises with activities.
The client must be encouraged to assume increasing participation in self-care activities. The client is taught to coordinate diaphragmatic breathing with activities such as walking, bathing, bending, or climbing stairs. The client should bathe, dress, and take short walks, resting as needed to avoid fatigue and excessive dyspnea.
Perform postural drainage as indicated.
If the management of secretions is a problem, postural drainage may be performed to allow the secretions to be drained. Postural drainage is used to prevent or relieve bronchial obstruction caused by the accumulation of secretions. Several positions are used so that the force of gravity helps move secretions from the smaller bronchial airways to the main bronchi and trachea.
Instruct the client on how to use an incentive spirometer.
Incentive spirometry is a method of deep breathing that provides visual feedback to encourage the client to inhale slowly and deeply to maximize lung inflation.
- The client assumes a semi-Fowler or a sitting position to enhance diaphragmatic excursion.
- Instruct the client to use diaphragmatic breathing techniques.
- The nurse instructs the client to place the mouthpiece of the spirometer firmly in the mouth, breathe in the air slowly through the mouth, and hold their breath at the end of inspiration for about three seconds to maintain the ball between the lines.
- The client exhales slowly through the mouthpiece.
- Instruct the client to cough during and after each session.
- Perform the procedure approximately 10 times in succession, repeating the 10 breaths with the spirometer each hour during waking hours.
Administer oxygen therapy as indicated.
Oxygen therapy can be given as long-term continuous therapy, during exercise, or to prevent acute dyspnea during an exacerbation. For clients with exercise-induced hypoxemia, oxygen supplementation during exercise may improve performance. Intermittent oxygen therapy is indicated for clients who desaturate only during activities of daily living, exercise, or sleep.
Encourage the client to participate in pulmonary rehabilitation.
Pulmonary rehabilitation id clients with chronic pulmonary diseases such as COPD is well-established and widely accepted as a means to alleviate symptoms and optimize functional status. Pulmonary rehabilitation includes assessment, education, smoking cessation, physical reconditioning, nutritional counseling, skills training, and psychological support. Breathing exercises, as well as retraining and exercise programs, are used to improve functional status.
Encourage the client to perform physical activities as tolerated.
Physical conditioning techniques include breathing exercises and general exercises intended to conserve energy and increase pulmonary ventilation. Graded exercises and physical conditioning programs using treadmills, stationary bicycles, and measured-level walks can improve symptoms and increase work capacity and exercise tolerance. Any physical activity that can be performed regularly is helpful.
Assist the client with coping measures.
Any factor that interferes with normal breathing quite naturally induces anxiety, depression, and changes in behavior. Restricted activity and reversal of family roles due to loss of employment, the frustration of having to work to breathe, and the realization that the disease is prolonged and unrelenting may cause the client to become angry, depressed, and demanding.
For clients with cardiovascular problems
Place the client in bed rest as recommended.
Bed or chair rest during the initial phase of treatment in a client with MI helps reduce myocardial oxygen consumption. The limitation on mobility should remain until the client is pain-free and hemodynamically stable.
Administer pain medications such as nitroglycerin as prescribed.
The pain associated with an acute MI reflects an imbalance in myocardial oxygen supply and demand or ineffective myocardial tissue perfusion. Promptly relieving the pain helps to reestablish this balance, thus increasing the workload of the heart and allowing the client to gradually start their usual activities as tolerated.
Refer the client to cardiac rehabilitation.
Cardiac rehabilitation is an important continuing care program for clients with coronary artery disease that targets risk reduction by providing client and family education, offering individual and group support, and encouraging physical activity and physical conditioning. The goals are to extend life and improve the quality of life.
Aid the client during physical conditioning.
Physical conditioning is achieved gradually over time. Many times, clients will “overdo it” in an attempt to achieve their goals too rapidly. Observe the client for chest pain, dyspnea, weakness, fatigue, and palpitations and instruct them to stop exercise if any of these occur.
Alternate the client’s rest with activity periods.
The nurse plans the client’s activities so that they occur in cycles alternating rest with their activity. This improves the client’s physiologic status, and it helps educate the client about the need for planned cycles of rest and activity. The client may sit and read a newspaper or engage in relaxing activities after taking a bath or shower. The client should avoid having two significant energy-consuming activities on the same day or in immediate succession.
Assist the client in managing emotional responses to their disease.
The client is assisted in identifying things in life that they had lost and their emotional responses to the loss. The nurse then assists the client in identifying the amount of control that they still have over life, such as making food choices, managing medications, and working with the healthcare provider to achieve the best possible outcomes.
Provide a low-sodium diet.
Following a low-sodium (no more than 2 g/day) diet and avoiding excessive fluid intake are usually recommended for clients with heart failure, decreasing dietary sodium reduces fluid retention and the on symptoms of peripheral and pulmonary congestion. The purpose of sodium restriction is to decrease the amount of circulating blood volume, which decreases myocardial work. Client adherence is important because dietary indiscretions may result in severe exacerbations of HF requiring hospitalization.
Administer oxygen therapy as prescribed.
Oxygen therapy may be necessary as heart failure progresses. The need is based on the degree of pulmonary congestion and resulting hypoxia. Some clients require supplemental oxygen only during periods of activity.
Encourage regular physical activity as recommended.
The reduced physical activity caused by HF symptoms leads to physical deconditioning that worsens the client’s symptoms and exercise tolerance. A typical program for a client with HF might include a daily walking regimen, with the duration increased over a 6-week period. Because some clients may be severely debilitated, they need to limit physical activities to only three to five minutes at a time, one to four times per day.
Recommend methods to adjust a client’s daily activity.
Instruct clients on some methods of adjusting an activity. For example, vegetables can be chopped or peeled while sitting at the kitchen table rather than standing at the kitchen counter. Small frequent meals decrease the amount of energy needed for digestion while providing adequate nutrition. The client may prepare meals for the entire day during the morning.
Monitor the client’s response to activities.
The client’s response needs to be monitored. If the client is hospitalized, vital signs and oxygen saturation levels are monitored before, during, and immediately after an activity to identify whether they are within the desired range. If the client is at home, the degree of fatigue felt after the activity can be used to assess the response.
For clients with insufficient circulation and blood-borne pathologies
Monitor the client’s level of fatigue.
The most common symptom and complication of anemia is fatigue. Fatigue is often the symptom that has the greatest negative impact on a client’s level of functioning and consequent quality of life. Fatigue can interfere with a client’s ability to work and participate in activities with family and friends. Clients often lose interest in hobbies and activities, including sexual activity.
Assist the client in balancing periods of rest and activity.
Nursing interventions for a client with chronic anemia can focus on assisting the client to prioritize activities and establish a balance between activity and rest that is acceptable to the client. The distress from fatigue is often related to a client’s responsibilities and life demands as well as the amount of assistance and support received from others.
Advise the client about maintaining adequate nutrition.
Inadequate intake of essential nutrients, such as iron, vitamin B12, folic acid, and protein, can cause some anemias. The symptoms associated with anemia, such as fatigue and anorexia, can in turn interfere with maintaining adequate nutrition. Dietary supplements such as vitamins, iron, folate, and protein may be prescribed.
Provide an environment conducive to rest and sleep.
Sleep disturbance can exacerbate fatigue. Maintain a comfortable room temperature that is neither too hot nor too cold. Consider using white noise machines or earplugs to block out disruptive sounds that might interfere with the client’s sleep. Encourage the client to maintain a consistent sleep schedule. This can help regulate the body’s internal clock.
Encourage the client to perform self-care activities on their own.
The client should be encouraged to do as much as possible to preserve mobility and function as well as self-esteem. Clients may have negative feelings because they can no longer care for themselves. As the client recovers, the nurse may assist them to resume more self-care.
Promote activities that improve physical conditioning.
A client with acute leukemia needs to maintain some physical activity and exercise to prevent the deconditioning that results from inactivity. The use of a high-efficiency particulate air (HEPA) filter mask can allow the client to ambulate outside their room despite severe neutropenia. Stationary bicycles may also be set up in the room. At a minimum, the client may be encouraged to sit up in a chair while awake rather than staying in bed.
Provide small, frequent meals and healthy snacks.
Small, frequent feedings of foods that are soft in texture and moderate in temperature may be better tolerated. To keep the client’s energy increased, eating smaller meals and healthy snacks every three to four hours, rather than large meals can help regain physical limitations (Barhum & Fogoros, 2021).
Instruct the client to reduce consumption of caffeine and alcohol.
Cutting down on caffeine may help the client feel less tired. Caffeine can be found in coffees, teas, colas, energy drinks, pain medications, and herbal supplements. Avoiding alcohol may also improve the client’s energy levels, as it helps with falling asleep but can cause less sleep after consuming it.
Administer blood and blood products as indicated.
Clients with acute blood loss or severe hemolysis may not tolerate typical activities because of decreased blood volume or reduced circulating erythrocytes. Lost volume is replaced with transfusions of intravenous fluids, based on symptoms and laboratory test results. RBC transfusions have been shown to be highly effective in several situations; in an acute exacerbation of anemia, in the prevention of severe complications from anesthesia and surgery, in improving response to infection, and in preventing cerebral edema in stroke.
Administer pain medications as prescribed.
Pain management is a significant issue for clients with sickle cell disease. The severity of pain may not be enough to cause the client to seek assistance from healthcare providers but severe enough to interfere with the ability to work and function within the family unit. Aspirin is very useful in diminishing mild to moderate pain; it also diminishes inflammation and potential thrombosis. NSAIDs are useful for moderate pain or in combination with opioid analgesics.
3. Providing Client and Caregiver Education
Clients may lack knowledge about managing their condition and activity levels. The nurse should provide education on energy conservation techniques, proper medication management, lifestyle modifications, and when to seek medical assistance.
Teach the client and/or SO to recognize signs of physical overactivity or overexertion.
Knowledge promotes awareness to prevent the complication of overexertion. Clients with COPD present with dyspnea during exercise, which progresses to dyspnea at rest upon exacerbation of the disease. Work of breathing increases over time and accessory muscles are recruited in an effort to breathe. Activity-induced angina or shortness of breath may indicate coronary artery disease, which requires medical attention.
Teach energy conservation techniques.
The nurse can help the client reduce activity limitations by planning self-care activities and determining the best times for bathing, dressing, and other daily activities. These techniques can help reduce oxygen consumption, allowing a more prolonged activity. These may include:
- Sitting to do tasks
- Frequent position changes
- Pushing rather than pulling
- Sliding rather than lifting
- Working at an even pace
- Placing frequently used items within easy reach
- Resting for at least 1 hour after meals before starting a new activity
- Using wheeled carts for laundry, shopping, and cleaning needs
- Organizing a work-rest-work schedule
Educate clients and caregivers about the disease process and therapeutic management.
Most clients cope better when they understand what is happening to them. Based on their health literacy level, and interest, education of the client and their family should begin with a focus on the disease, including some pathophysiology, and its treatment.
Inform the client and family about the proper use of nutritional supplements.
The client and family must understand the role of nutritional supplements in the proper context because many forms of anemia are not the result of nutrient deficiencies. Even an excessive intake of nutritional supplements will not improve anemia.
Instruct the client with COPD to avoid extremes of temperature.
The nurse instructs the client to avoid extremes of heat and cold. Heat increases the body temperature, thereby raising oxygen requirements, and cold tends to promote bronchospasm. Air pollutants such as fumes, smoke, dust, and even talcum, lint, and aerosol sprays may initiate bronchospasm. High altitudes aggravate hypoxemia.
Provide referrals to home and community-based care.
Referral for home, community-based, or transitional care is important to enable assessment of the client’s home environment and physical and psychological status, to evaluate the client’s adherence to a prescribed regimen, and to assess the client’s ability to cope with changes in lifestyle and physical status.
Recommended Resources
Recommended nursing diagnosis and nursing care plan books and resources.
Disclosure: Included below are affiliate links from Amazon at no additional cost from you. We may earn a small commission from your purchase. For more information, check out our privacy policy.
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care
We love this book because of its evidence-based approach to nursing interventions. This care plan handbook uses an easy, three-step system to guide you through client assessment, nursing diagnosis, and care planning. Includes step-by-step instructions showing how to implement care and evaluate outcomes, and help you build skills in diagnostic reasoning and critical thinking.

Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition)
Includes over two hundred care plans that reflect the most recent evidence-based guidelines. New to this edition are ICNP diagnoses, care plans on LGBTQ health issues, and on electrolytes and acid-base balance.

Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales
Quick-reference tool includes all you need to identify the correct diagnoses for efficient patient care planning. The sixteenth edition includes the most recent nursing diagnoses and interventions and an alphabetized listing of nursing diagnoses covering more than 400 disorders.

Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care
Identify interventions to plan, individualize, and document care for more than 800 diseases and disorders. Only in the Nursing Diagnosis Manual will you find for each diagnosis subjectively and objectively – sample clinical applications, prioritized action/interventions with rationales – a documentation section, and much more!

All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health
Includes over 100 care plans for medical-surgical, maternity/OB, pediatrics, and psychiatric and mental health. Interprofessional “patient problems” focus familiarizes you with how to speak to patients.

References
Suggested resources and references to enhance your understanding of this activity intolerance nursing care plan.
- de Souza, V., Salloum Zeitoun, S., Takao Lopes, C., Dias de Oliveira, A. P., de Lima Lopes, J., & Bottura Leite de Barros, A. L. (2015). Clinical usefulness of the definitions for defining characteristics of activity intolerance, excess fluid volume and decreased cardiac output in decompensated heart failure: a descriptive exploratory study. Journal of Clinical Nursing, 24(17-18), 2478-2487.
- Hur, H. K., Park, S. M., Kim, S. S., Storey, M. J., & Kim, G. Y. (2005). Activity intolerance and impaired physical mobility in elders. International Journal of Nursing Terminologies and Classifications, 16(3‐4), 47-53.
- Rodrigues, C. G., Moraes, M. A., Sauer, J. M., Kalil, R. A. K., & de Souza, E. N. (2011). Nursing diagnosis of activity intolerance: clinical validation in patients with refractory angina. International Journal of Nursing Terminologies and Classifications, 22(3), 117-122.
- Andriani, W. R., Suwanto, A. W., Wiratmoko, H., Hartanto, A. E., Antono, S. D., Purwaningsih, E., Hendrawati, G. W., Failasufi, M., & Cahyono, L. (2022). Exercise Habits and Family Disease History as Determinant of Activity Intolerance and ECG Patterns of Patients with Acute Coronary Syndrome (ACS). Health Notions, 6(4).
- Barhum, L., & Fogoros, R. N. (2021, July 1). Iron Deficiency Anemia: Coping, Support, and Living Well. Verywell Health.
- Buzaid, A., Dodge, M. P., Handmacher, L., & Kiltz, P. J. (2013). Activities of Daily Living Evaluation and Treatment in Persons with Multiple Sclerosis. Physical Medicine and Rehabilitation Clinics of North America, 24(4).
- Hanania, N. A., & O’Donnell, D. E. (2019). Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. International Journal of Chronic Obstructive Pulmonary Disease, 14.
- Hinkle, J. L., & Cheever, K. H. (2018). Brunner & Suddarth’s Textbook of Medical-surgical Nursing. Wolters Kluwer.
- Shalahuddin, I., Nugraha, B. A., Pebrianti, S., Eriyani, T., & Nurrahmawati, D. (2022). Activity Intervention in COPD Patients to Improve Quality of Life in The Comunity. Jurnal Aisyah: Jurnal Ilmu Kesehatan, 7(4).
- Thibault, P., Loisel, P., Durand, M.-J., Catchlove, R., & Sullivan, M. J.L. (2008). Psychological predictors of pain expression and activity intolerance in chronic pain patients. PAIN, 139(1).
























Leave a Comment