Learn about the nursing care management of patients with hypertension.
What is Hypertension?
Hypertension is one of the most common lifestyle diseases to date. It affects people from all walks of life. Let us get to know hypertension more by its definitions.
- Hypertension is defined as a systolic blood pressure greater than 140 mmHg and a diastolic pressure of more than 90 mmHg.
- This is based on the average of two or more accurate blood pressure measurements during two or more consultations with the healthcare provider.
- The definition is taken from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.
Classification
In 2017, the American College of Cardiology and the American Heart Association revised their hypertension guidelines. The previous guidelines set the threshold at 140/90 mm Hg for younger people and 150/80 mm Hg for those ages 65 and older.
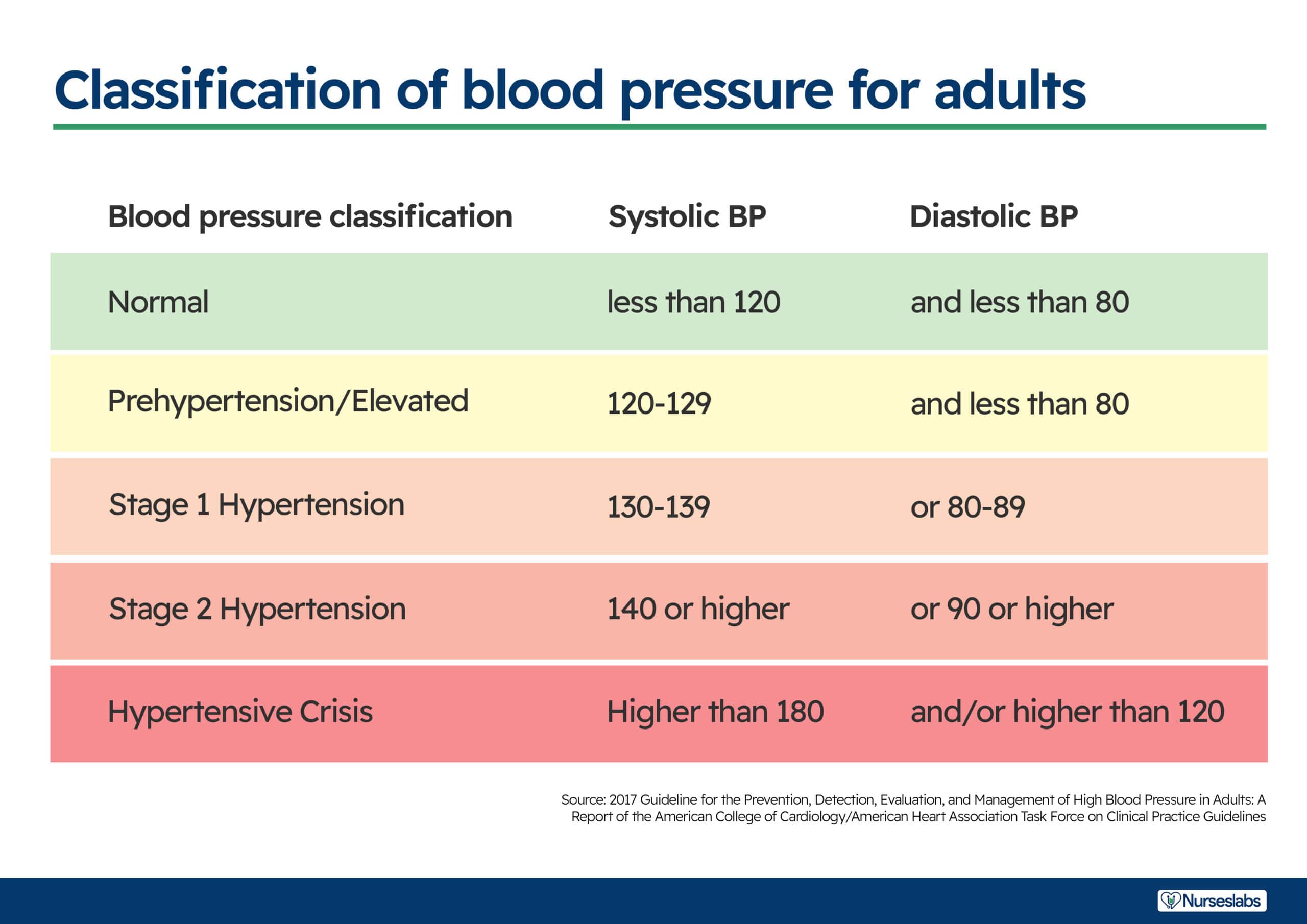
- Normal. The normal range for blood pressure is between, less than 120 mmHg and less than 80 mmHg.
- Elevated. Elevated stage starts from 120 mmHg to 129 mmHg for systolic blood pressure and less than 80 mmHg for diastolic pressure.
- Stage 1 hypertension. Stage 1 starts when the patient has a systolic pressure of 130 to 139 mmHg and a diastolic pressure of 80 to 89 mmHg.
- Stage 2 hypertension. Stage 2 starts when the systolic pressure is already more than or equal than 140 mmHg and the diastolic is more than or equal than 90 mmHg.
Pathophysiology
In a normal circulation, pressure is transferred from the heart muscle to the blood each time the heart contracts and then pressure is exerted by the blood as it flows through the blood vessels.
The pathophysiology of hypertension follows.
- Hypertension is a multifactorial
- When there is excess sodium intake, renal sodium retention occurs, which increases fluid volume resulting in increased preload and increase in contractility.
- Obesity is also a factor in hypertension because hyperinsulinemia develops and structural hypertrophy results leading to increased peripheral vascular resistance.
- Genetic alteration also plays a role in the development of hypertension because when there is cell membrane alteration, functional constriction may follow and also results in increased peripheral vascular resistance.
Epidemiology
Hypertension is slowly rising to the top as one of the primary causes of morbidity in the world. Here are the current statistics of the status of hypertension in some of the leading countries.
- About 31% of the adults in the United States have hypertension.
- African-Americans have the highest prevalence rate of 37%.
- In the total US population of persons with hypertension, 90% to 95% have primary hypertension or high blood pressure from an unidentified cause.
- The remaining 5% to 10% of this group have secondary hypertension or high blood pressure related to identified causes.
- Hypertension is also termed as the “silent killer” because 24% of people who had pressures exceeding 140/90 mmHg were unaware that their blood pressures were elevated.
Causes
Hypertension has a lot of causes just like how fever has many causes. The factors that are implicated as causes of hypertension are:
- Increased sympathetic nervous system activity. Sympathetic nervous system activity increases because there is dysfunction in the autonomic nervous system.
- Increase renal reabsorption. There is an increase reabsorption of sodium, chloride, and water which is related to a genetic variation in the pathways by which the kidneys handle sodium.
- Increased RAAS activity. The renin-angiotensin-aldosterone system increases its activity leading to the expansion of extracellular fluid volume and increased systemic vascular resistance.
- Decreased vasodilation of the arterioles. The vascular endothelium is damaged because of the decrease in the vasodilation of the arterioles.
Clinical Manifestations
Many people who have hypertension are asymptomatic at first. Physical examination may reveal no abnormalities except for an elevated blood pressure, so one must be prepared to recognize hypertension at its earliest.
- Headache. The red blood cells carrying oxygen is having a hard time reaching the brain because of constricted vessels, causing headache.
- Dizziness occurs due to the low concentration of oxygen that reaches the brain.
- Chest pain. Chest pain occurs also due to decreased oxygen levels.
- Blurred vision. Blurred vision may occur later on because of too much constriction in the blood vessels of the eye that red blood cells carrying oxygen cannot pass through.
Prevention
Prevention of hypertension mainly relies on a healthy lifestyle and self-discipline.
- Weight reduction. Maintenance of normal body weight can help prevent hypertension.
- Adopt DASH. DASH or the Dietary Approaches to Stop Hypertension includes consummation of a diet rich in fruits, vegetable, and low-fat dairy.
- Dietary sodium retention. Sodium contributes to an elevated blood pressure, so reducing the dietary intake to no more than 2.4 g sodium per day can be really helpful.
- Physical activity. Engage in regular aerobic physical activity for 30 minutes thrice every week.
- Moderation of alcohol consumption. Limit alcohol consumption to no more than 2 drinks per day in men and one drink for women and people who are lighter in weight.
Complications
If hypertension is left untreated, it could progress to complications of the different body organs.
- Heart failure. With increased blood pressure, the heart pumps blood faster than normal until the heart muscle goes weak from too much exertion.
- Myocardial infarction. Decreased oxygen due to constriction of blood vessels may lead to MI.
- Impaired vision. Ineffective peripheral perfusion affects the eye, causing problems in vision because of decreased oxygen.
- Renal failure. Blood carrying oxygen and nutrients could not reach the renal system because of the constricted blood vessels.
Assessment and Diagnostic Findings
Assessment of the patient with hypertension must be detailed and thorough. There are also diagnostic tests that can be performed to establish the diagnosis of hypertension.
Assessment
- Assess the patient’s health history
- Perform physical examination as appropriate.
- The retinas are examined to assess possible organ damage.
- Laboratory tests are also taken to check target organ damage.
Diagnostic Tests
- Urinalysis is performed to check the concentration of sodium in the urine though the specific gravity.
- Blood chemistry (e.g. analysis of sodium, potassium, creatinine, fasting glucose, and total and high density lipoprotein cholesterol levels). These tests are done to determine the level of sodium and fat in the body.
- 12-lead ECG. ECG needs to be performed to rule presence of cardiovascular damage.
- Echocardiography. Echocardiography assesses the presence of left ventricular hypertrophy.
- Creatinine clearance. Creatinine clearance is performed to check for the level of BUN and creatinine that can determine if there is renal damage or not.
- Renin level. Renin level should be assessed to determine how RAAS is coping.
- Hemoglobin/hematocrit: Not diagnostic but assesses relationship of cells to fluid volume (viscosity) and may indicate risk factors such as hypercoagulability, anemia.
- Blood urea nitrogen (BUN)/creatinine: Provides information about renal perfusion/function.
- Glucose: Hyperglycemia (diabetes mellitus is a precipitator of hypertension) may result from elevated catecholamine levels (increases hypertension).
- Serum potassium: Hypokalemia may indicate the presence of primary aldosteronism (cause) or be a side effect of diuretic therapy.
- Serum calcium: Imbalance may contribute to hypertension.
- Lipid panel (total lipids, high-density lipoprotein [HDL], low-density lipoprotein [LDL], cholesterol, triglycerides, phospholipids): Elevated level may indicate predisposition for/presence of atheromatous plaques.
- Thyroid studies: Hyperthyroidism may lead or contribute to vasoconstriction and hypertension.
- Serum/urine aldosterone level: May be done to assess for primary aldosteronism (cause).
- Urinalysis: May show blood, protein, or white blood cells; or glucose suggests renal dysfunction and/or presence of diabetes.
- Creatinine clearance: May be reduced, reflecting renal damage.
- Urine vanillylmandelic acid (VMA) (catecholamine metabolite): Elevation may indicate presence of pheochromocytoma (cause); 24-hour urine VMA may be done for assessment of pheochromocytoma if hypertension is intermittent.
- Uric acid: Hyperuricemia has been implicated as a risk factor for the development of hypertension.
- Renin: Elevated in renovascular and malignant hypertension, salt-wasting disorders.
- Urine steroids: Elevation may indicate hyperadrenalism, pheochromocytoma, pituitary dysfunction, Cushing’s syndrome.
- Intravenous pyelogram (IVP): May identify cause of secondary hypertension, e.g., renal parenchymal disease, renal/ureteral calculi.
- Kidney and renography nuclear scan: Evaluates renal status (TOD).
- Excretory urography: May reveal renal atrophy, indicating chronic renal disease.
- Chest x-ray: May demonstrate obstructing calcification in valve areas; deposits in and/or notching of aorta; cardiac enlargement.
- Computed tomography (CT) scan: Assesses for cerebral tumor, CVA, or encephalopathy or to rule out pheochromocytoma.
- Electrocardiogram (ECG): May demonstrate enlarged heart, strain patterns, conduction disturbances. Note: Broad, notched P wave is one of the earliest signs of hypertensive heart disease.
Medical Management
Main Topic: Antihypertensive Drugs
The goal of hypertension treatment is to prevent complications and death by achieving and maintaining arterial blood pressure at or below 130/80 mmHg.
Pharmacologic Therapy
- The medications used for treating hypertension decrease peripheral resistance, blood volume, or the strength and rate of myocardial contraction.
- For uncomplicated hypertension, the initial medications recommended are diuretics and beta blockers.
- Only low doses are given, but if blood pressure still exceeds 140/90 mmHg, the dose is increased gradually.
- Thiazide diuretics decrease blood volume, renal blood flow, and cardiac output.
- ARBs are competitive inhibitors of aldosterone binding.
- Beta blockers block the sympathetic nervous system to produce a slower heart rate and a lower blood pressure.
- ACE inhibitors inhibit the conversion of angiotensin I to angiotensin II and lowers peripheral resistance.
Stage 1 Hypertension
- Thiazide diuretic is recommended for most and angiotensin-converting enzyme-1, aldosterone receptor blocker, beta blocker, or calcium channel blocker is considered.
Stage 2 Hypertension
- Two-drug combination is followed, usually including thiazide diuretic and angiotensin-converting enzyme-1, or beta-blocker, or calcium channel blocker.
Nursing Management
The goal of nursing management is to help achieve a normal blood pressure through independent and dependent interventions.
Nursing Assessment
Nursing assessment must involve careful monitoring of the blood pressure at frequent and routinely scheduled intervals.
- If patient is on antihypertensive medications, blood pressure is assessed to determine the effectiveness and detect changes in the blood pressure.
- Complete history should be obtained to assess for signs and symptoms that indicate target organ damage.
- Pay attention to the rate, rhythm, and character of the apical and peripheral pulses.
Diagnosis
Based on the assessment data, nursing diagnoses may include the following:
- Deficient knowledge regarding the relation between the treatment regimen and control of the disease process.
- Noncompliance with the therapeutic regimen related to side effects of the prescribed therapy.
- Risk for activity intolerance related to imbalance between oxygen supply and demand.
- Risk-prone health behavior related to condition requiring change in lifestyle.
Nursing Care Plan and Goals
Main article: Hypertension Nursing Care Plans
The major goals for a patient with hypertension are as follows:
- Understanding of the disease process and its treatment.
- Participation in a self-care program.
- Absence of complications.
- BP within acceptable limits for individual.
- Cardiovascular and systemic complications prevented/minimized.
- Disease process/prognosis and therapeutic regimen understood.
- Necessary lifestyle/behavioral changes initiated.
- Plan in place to meet needs after discharge.
Nursing Priorities
- Maintain/enhance cardiovascular functioning.
- Prevent complications.
- Provide information about disease process/prognosis and treatment regimen.
- Support active patient control of condition.
Nursing Interventions
The objective of nursing care focuses on lowering and controlling the blood pressure without adverse effects and without undue cost.
- Encourage the patient to consult a dietitian to help develop a plan for improving nutrient intake or for weight loss.
- Encourage restriction of sodium and fat
- Emphasize increase intake of fruits and vegetables.
- Implement regular physical activity.
- Advise patient to limit alcohol consumption and avoidance of tobacco.
- Assist the patient to develop and adhere to an appropriate exercise regimen.
Evaluation
At the end of the treatment regimen, the following are expected to be achieved:
- Maintain blood pressure at less than 140/90 mmHg with lifestyle modifications, medications, or both.
- Demonstrate no symptoms of angina, palpitations, or visual changes.
- Has stable BUN and serum creatinine levels.
- Has palpable peripheral pulses.
- Adheres to the dietary regimen as prescribed.
- Exercises regularly.
- Takes medications as prescribed and reports side effects.
- Measures blood pressure routinely.
- Abstains from tobacco and alcohol intake.
- Exhibits no complications.
Discharge and Home Care Guidelines
Following discharge, the nurse should promote self-care and independence of the patient.
- The nurse can help the patient achieve blood pressure control through education about managing blood pressure.
- Assist the patient in setting goal blood pressures.
- Provide assistance with social support.
- Encourage the involvement of family members in the education program to support the patient’s efforts to control hypertension.
- Provide written information about expected effects and side effects.
- Encourage and teach patients to measure their blood pressures at home.
- Emphasize strict compliance of follow-up check up.
Documentation Guidelines
These are the following data that should be documented for the patient’s record:
- Effects of behavior on health status/condition.
- Plan for adjustments and interventions for achieving the plan and the people involved.
- Client responses to the interventions, teaching, and action plan performed.
- Attainment or progress towards desired outcome.
- Modifications to plan care.
- Individual findings including deviation from prescribed treatment plan.
- Consequences of actions to date.
See Also
Posts related to Hypertension:

























Leave a Comment