
Get to learn about the nursing care management for patients with cancer in this study guide.
Epidemiology
Overall, the incidence of cancer is higher in men than in women and higher in industrialized sectors and nations.
- More than 1.4 million Americans are diagnosed each year with cancer, affecting one of various body sites.
- Cancer is second only to cardiovascular disease as a leading cause of death in the United States.
- Although the number of cancer deaths has decreased slightly, more than 560, 000 Americans were expected to die from a malignant process in 2008.
- The leading causes of cancer deaths in the United States, in order of frequency, are lung, prostate, and colorectal cancer in men and lung, breast, and colorectal cancer women.
- For all cancer sites combined, African American men have a 15% higher incidence rate and a 38% higher death rate than Caucasian men.
African-American women have a 9% lower incidence rate, but an 18% higher death rate than Caucasian women for all cancer sites combined.
Pathophysiology
Cancer is a disease process that begins when an abnormal cell is transformed by the genetic mutation of the cellular DNA.
- Proliferative patterns. Cancerous cells are described as malignant neoplasms because they demonstrate uncontrolled cellular growth that follows no physiologic demand (neoplasia).
- Characteristics of malignant cells. Cells are undifferentiated and often bear little resemblance to the normal cells; they grow at the periphery and sends out processes that infiltrate and destroy the surrounding tissues; the rate of their growth is variable and depends on level of differentiation; they can gain access to the blood and lymphatic channels and metastasizes to other areas of the body; they often cause generalized effects such as anemia, weakness, and weight loss; they often cause extensive tissue damage and causes death unless growth can be controlled.
- Invasion and metastasis. Malignant disease processes have the ability to allow the spread or transfer of cancerous cells from one organ or body part to another by invasion (growth of the primary tumor into the surrounding host tissues) and metastasis (dissemination or spread of malignant cells from the primary tumor to distant sites.
- Carcinogenesis. Carcinogenesis is a malignant transformation that involves initiation (initiators such as chemicals, physical factors, and biologic agents, escape normal enzymatic mechanisms and alter the genetic structure of the cellular DNA), promotion (repeated exposure to carcinogens causes the expression of abnormal or mutant genetics information), and progression (the altered cells exhibit increased malignant behavior).
- Role of the immune system. Some evidence indicates that the immune system can detect the development of malignant cells and destroy them before cell growth becomes uncontrolled, but when the immune system fails to identify and stop the growth of malignant cells, clinical cancer develops.
Detection and Prevention of Cancer
Nurses and physicians have traditionally been involved with tertiary prevention, the care, and rehabilitation of patients after cancer diagnosis and treatment, but the American Cancer Society, the National Cancer Institute, clinicians, and researchers also place emphasis on primary and secondary prevention of cancer.
- Primary prevention. Primary prevention is concerned with reducing risks of disease through health promotion strategies.
- Secondary prevention. Secondary prevention programs promote screening and early detection activities such as breast and testicular self-examination and Papanicolaou (Pap) tests.
Diagnosis of Cancer
A cancer diagnosis is based on the assessment of physiologic and functional changes and results of the diagnostic evaluation.
- Tumor marker identification. Analysis of substances found in body tissues, blood or other body fluids that are made by the tumor or by the body in response to the tumor.
- Genetic profiling. Analysis for the presence of mutations in genes found in tumors or body tissues.
- Mammography. Mammography is the use of x-ray images of the breast.
- Magnetic resonance imaging (MRI). MRI uses magnetic fields and radio-frequency signals to create sectioned images of various body structures.
- Computed tomography (CT). CT scan uses narrow-beam x-ray to scan successive layers of tissue for a cross-sectional view.
- Fluoroscopy. Use of X-rays that identify contrasts in the body tissue densities; may involve the use of contrast agents.
- Ultrasonography. Ultrasound uses high-frequency sound waves echoing off body tissues and is converted electronically into images; used to assess deep tissues within the body.
- Endoscopy. Direct visualization of a body cavity or passageway by insertion of an endoscope into a body cavity or opening; allows tissue biopsy, fluid aspiration, and excision of small tumors.
- Nuclear medicine imaging. Uses intravenous injection or ingestion of radioisotope substances followed by imaging of tissues that have concentrated the radioisotopes.
- Positron emission tomography (PET). Through the use of a tracer, provides black and white or color-coded images of the biologic activity of a particular area, rather than its structure.
- PET fusion. Use of a PET scanner and a CT scanner in one machine to provide an image combining anatomic detail, spatial resolution, and functional metabolic abnormalities.
- Radioimmunoconjugates. Monoclonal antibodies are labeled with a radioisotope and injected intravenously into the patient.
Tumor Staging and Grading
A complete diagnostic evaluation include identifying the stage and grade of the tumor.
Staging. Staging determines the size of the tumor and the existence of local invasion and distant metastasis.
- Tumor, nodes, and metastasis (TNM) system. The TNM system is frequently used, where T is the extent of the primary tumor, N is the absence or presence and extent of regional lymph node metastasis, and M is the absence or presence of distant metastasis.
- Grading. Grading refers to the classification of the tumor cells, and it seeks to define the type of tissue from which the tumor originated and the degree to which the tumor cells retain the functional and histologic characteristics of the tissue of origin.
- Grade I to IV. Grade I tumors, also known as well-differentiated tumors, closely resemble the tissue of origin in structure and function while Grade IV tumors do not clearly resemble the tissue of origin in structure and function.
Management of Cancer
Treatment options offered to cancer patients should be based on treatment goals for each specific type of cancer.
Surgery
Surgical removal of entire cancer remains the ideal and most frequently used treatment method.
Diagnostic Surgery
Biopsy
- Biopsy. Biopsy is usually performed to obtain a tissue sample for analysis of the cells suspected to be malignant.
- Types of biopsy. The three most common biopsy methods are the excisional, incisional, and needle methods.
- Excisional biopsy. Excisional biopsy is most frequently used for easily accessible tumors of the skin, breast, and upper and lower gastrointestinal and upper respiratory tracts.
- Incisional biopsy. Incisional biopsy is performed if the tumor mass is too large to be removed.
- Needle biopsy. Needle biopsies are performed to sample suspicious masses that are easily accessible, such as growths in the breasts, thyroid, lung, liver, and kidney.
Surgery as Primary Treatment
When surgery is the primary approach in treating cancer, the goal is to remove the entire tumor or as much as is feasible and any involved surrounding tissue, including regional lymph nodes.
- Local excision. Local excision, often performed on an outpatient basis, is warranted when the mass is small, and it includes removal of the mass and a small margin of normal tissue that is easily accessible.
- Wide or radical excisions. Wide excisions include removal of the primary tumor, lymph nodes, adjacent involved structures, and surrounding tissues that may be at high risk for tumor spread.
- Video-assisted endoscopic surgery. In this minimally invasive procedure, an endoscope with intense lighting and an attached multichip mini-camera is inserted into the body through a small incision.
- Salvage surgery. Salvage surgery is an additional treatment option that is an extensive surgical approach to treat the local recurrence of cancer after the use of a less extensive primary approach.
- Electrosurgery. Uses electric current to destroy tumor cells.
- Cryosurgery. Uses liquid nitrogen or a very cold probe to freeze tissue and cause cell destruction.
- Chemosurgery. Uses chemicals or chemotherapy applied directly to the tissue to cause destruction.
- Laser surgery. Uses light and energy aimed at an exact tissue location and depth to vaporize cancer cells.
- Photodynamic therapy. Intravenous administration of a light-sensitizing agent that is taken up by cancer cells, followed by exposure to laser within 24-48 hours.
- Radiofrequency ablation. Uses localized application of thermal energy that destroys cancer cells through heat.
Prophylactic Surgery
Prophylactic surgery involves removing nonvital tissues or organs that are at increased risk to develop cancer.
- Examples of prophylactic surgery. Colectomy, mastectomy, and oophorectomy are examples of prophylactic surgery.
- Qualified patients. Prophylactic surgery is offered selectively to patients and discussed thoroughly with patients and families.
Palliative Surgery
When a cure is not possible, the goals of treatment are to make the patient as comfortable as possible.
- Palliative surgery. Palliative surgery is performed in an attempt to relieve complications of cancer.
- Communication. Honest and informative communication with the patient and family about the goal of surgery is essential to avoid false hope and disappointment.
Reconstructive Surgery
Reconstructive surgery may follow curative or radical surgery.
- Reconstructive surgery. Reconstructive surgery may be performed in an attempt to improve function or obtain a more desirable cosmetic effect.
- Indications. Reconstructive surgery may be indicated for breast, head and neck, and skin cancers.
Radiation Therapy
More than half of patients with cancer receive a form of radiation therapy at some point during treatment.
- Uses. Radiation may be used to cure cancer, as in thyroid carcinomas, localized cancers of the head and neck, and cancers of the uterine cervix; it may control malignant disease when a tumor cannot be removed surgically or when local nodal metastasis is present, or it can be used neoadjuvantly.
- Types. Two types of ionizing radiation-electromagnetic radiation (xrays and gamma rays) and particulate radiation (electrons, beta particles, protons, neutrons, and alpha particles)- can lead to tissue disruption.
Radiation Dosage
Radiation dosage depends on the sensitivity of the target tissues to radiation, the size of the tumor, tissue tolerance of the surrounding normal tissues, and critical structures adjacent to the tumor target.
- Lethal tumor dose. The lethal tumor dose is defined as that dose that will eradicate 95% of the tumor yet preserve normal tissue.
- Fractions. In external beam radiation, the total radiation dose is delivered over several weeks in daily doses called fractions.
- Fractionated doses. Repeated radiation treatments over time also allow for the periphery of the tumor to be reoxygenated repeatedly, because tumors shrink from the outside inward.
Administration of Radiation
Radiation therapy can be administered in a variety of ways depending on the source of radiation used, the location of the tumor, and the type of cancer targeted.
- Teletherapy (external beam radiation). External beam radiation therapy is the most commonly used form of radiation, in which, depending on the size, shape, and location of the tumor, different energy levels are generated to produce a carefully shaped beam that will destroy the targeted tumor, yet spare the surrounding healthy tissues and organs in an effort to reduce the treatment toxicities for the patient.
- Brachytherapy (internal radiation). Internal radiation implantation, or brachytherapy, delivers a high dose of radiation to a localized area and can be implanted by means of needles, seeds, beads, or catheters into body cavities (vagina, abdomen, pleura) or interstitial compartments (breast, prostate).
Toxicity
- Alopecia. Altered skin integrity is a common effect and can include alopecia or hair loss.
- Stomatitis. Alterations in oral mucosa secondary to radiation therapy include stomatitis or inflammation of the oral tissues, xerostomia or dryness of the mouth, change and loss of taste, and increased salivation.
- Thrombocytopenia. Bone marrow cells proliferate rapidly, and if sites containing bone marrow are included in the radiation field, anemia, leukopenia, and thrombocytopenia may result.
Nursing Management in Radiation Therapy
- Assessment. The nurse assesses the patient’s skin and oropharyngeal mucosa regularly when radiation therapy is directed to these areas, and also the nutritional status and general well-being should be assessed.
- Symptoms. If systemic symptoms, such as weakness and fatigue, occur, the nurse explains that these symptoms are a result of the treatment and do not represent deterioration or progression of the disease.
- Safety precautions. Safety precautions used in caring for a patient receiving brachytherapy include assigning the patient to a private room, posting appropriate notices about radiation safety precautions, having staff members wear dosimeter badges, making sure that pregnant staff members are not assigned to the patient’s care, prohibiting visits by children and pregnant visitors, limiting visits from others to 30 minutes daily, and seeing that visitors maintain a 6 foot distance from the radiation source.
Chemotherapy
In chemotherapy, antineoplastic agents are used in an attempt to destroy tumor cells by interfering with cellular functions, including replication.
- Goal. The goal of treatment is the eradication of enough tumor so that the remaining tumor cells can be destroyed by the body’s immune system.
- Proliferating cells. Actively proliferating cells within a tumor are the most sensitive to chemotherapeutic agents.
- Nondividing cells. Nondividing cells capable of future proliferation are the least sensitive to antineoplastic medications and consequently are potentially dangerous.
- Cell cycle-specific. Cell cycle-specific agents destroy cells that are actively reproducing by means of the cell-cycle; most affect cells in the S phase by interfering with DNA and RNA synthesis.
- Cell cycle-nonspecific. Chemotherapeutic agents that act independently of the cell cycle phases are cell cycle nonspecific, and they usually have a prolonged effect on cells, leading to cellular damage and death.
Antineoplastic Agents
Chemotherapeutic agents are also classified by chemical group, each with a different mechanism of action.
- Alkylating agents. Alters DNA structure by misreading DNA code, initiating breaks in the DNA molecule, cross-linking DNA strands
- Nitrosoureas. Similar to the alkylating agents, but they can cross the blood-brain barrier.
- Topoisomerase I inhibitors. Induce breaks in the DNA strand by binding to enzyme topoisomerase I, preventing cells from dividing.
- Antimetabolites. Antimetabolites interfere with the biosynthesis of metabolites or nucleic acids necessary for RNA and DNA synthesis.
- Antitumor antibiotics. Interfere with DNA synthesis by binding DNA and prevent RNA synthesis.
- Mitotic spindle poisons. Arrest metaphase by inhibiting mitotic tubular formation and inhibiting DNA and protein synthesis.
- Hormonal agents. Hormonal agents bind to hormone receptor sites that alter cellular growth; blocks binding of estrogens to receptor sites; inhibit RNA synthesis; suppress aromatase of P450 system, which decreases level.
Nursing Management in Chemotherapy
Nurses play an important role in assessing and managing many of the problems experienced by patients undergoing chemotherapy.
- Assessing fluid and electrolyte balance. Anorexia, nausea, vomiting, altered taste, mucositis, and diarrhea put patients at risk for nutritional and fluid electrolyte disturbances.
- Modifying risks for infection and bleeding. Suppression of the bone marrow and immune system is expected and frequently serves as a guide in determining appropriate chemotherapy dosage but increases the risk of anemia, infection, and bleeding disorders.
- Administering chemotherapy. The patient is observed closely during its administration because of the risk and consequences of extravasation, particularly of vesicant agent.
- Protecting caregivers. Nurses must be familiar with their institutional policies regarding personal protective equipment, handling and disposal of chemotherapeutic agents and supplies, and management of accidental spills or exposures.
Bone Marrow Transplantation
The role of bone marrow transplantation (BMT) for malignant and some nonmalignant diseases continues to grow.
Type of Bone Marrow Transplant
Types of BMT based on the source of donor cells include:
- Allogeneic. Allogeneic is from a related donor other than the patient; donor may be a related donor or a matched unrelated donor.
- Autologous. Autologous BMT is from the patient himself.
- Syngeneic. Syngeneic BMT is from an identical twin.
Nursing Management in Bone Marrow Transplantation
Nursing care of patients undergoing BMT is complex and demands a high level of skill.
- Implementing pretransplantation care. Nutritional assessments, extensive physical examinations, organ function tests, and psychological evaluations are conducted, with blood work that includes assessing past antigen exposure, and the patient’s support system, financial, and insurance resources are also evaluated.
- Providing care during treatment. Nursing management during bone marrow infusion or stem cell infusions consists of monitoring the patient’s vital signs and blood oxygen saturation; assessing for adverse effects such as fever, chills, shortness of breath, chest pain, cutaneous reactions, nausea, vomiting, hypotension, or hypertension, tachycardia, anxiety, and taste changes; and providing ongoing support and patient teaching.
- Providing posttransplantation care. Ongoing nursing assessments such as psychosocial assessments in follow-up visits are essential to detect late effects of therapy after BMT, which occur 100 days or more after the procedure, and donors also require nursing care through being assisted in maintaining realistic expectations of themselves as well as of the patient.
Targeted Therapies
Targeted therapies seek to minimize the negative effects on healthy tissues by disrupting specific cancer cell functions such as malignant transformation, cell communication pathways, processes for growth and metastasis, and genetic coding.
Biologic Response Modifiers (BRM)
Biologic response modifier therapy involves the use of naturally occurring or recombinant agents or treatment methods that can alter the immunologic relationship between the tumor and the host to provide a therapeutic benefit.
- Nonspecific biologic response modifiers. Nonspecific agents such as Calmette-Guérin (BCG) and Corynebacterium parvum, when injected into the patient, may serve as antigens that can stimulate an immune response in the hopes of eradicating malignant cells.
- Monoclonal antibodies. Monoclonal antibodies (MoAbs) have become available through technologic advances, and this type of specificity allows MoAbs to destroy the cancer cells and spare normal cells.
- Cytokines. Cytokines, substances produced by cells of the immune system to enhance the production and functioning of components of the immune system, are also the focus of cancer treatment research.
- Retinoids. Retinoids are vitamin A derivatives that play a role in growth, reproduction, apoptosis, epithelial cell differentiation, and immune function, wherein specific receptors in the cell nucleus are retinoid-dependent, thus when retinoids bind with these receptors, cell differentiation and replication are affected.
- Cancer vaccines. Cancer vaccines are used to mobilize the body’s immune response to recognize and attack cancer cells, as these cancer vaccines contain either portions of cancer cells alone or portions of cells in combination with other substances that can augment or boost immune responses.
Nursing Management in Biologic Response Modifier Therapy
It is essential for the nurse to assess the need for education, support, and guidance for both the patient and the family and assist in planning and evaluating patient care.
- Monitoring therapeutic and adverse effects. The nurse must be familiar with each agent given and its potential effects, and also, the nurse must be aware of the impact of these side effects on the patient’s quality of life.
- Promoting home and community-based care. The nurse teaches the patient and family how to administer BRMs through subcutaneous injections, provides instructions about side effects and helps the patient and family identify the strategies to manage many of the common side effects of BRM therapy.
Gene Therapy
Gene therapy includes approaches that correct genetic defects or manipulate genes to induce tumor cell destruction in the hope of preventing or combating the disease.
- Challenges. One of the challenges confronting cancer gene therapy is the multiple somatic mutations involved in the development of cancer, making it difficult to identify the most effective gene therapy approach.
- Viruses. Viruses used as vectors that transport a gene into a target cell via the cell membrane include retroviruses, adenoviruses, vaccinia virus, fowlpox, herpes simplex viruses, and Epstein-Barr viruses.
Approaches in Gene Therapy
Three general approaches have been used in the development of gene therapies, with adenoviruses showing effective promise in each approach.
- Tumor-directed therapy. This is the introduction of a therapeutic gene (suicide gene) into tumor cells in an attempt to destroy them.
- Active immunotherapy. Active immunotherapy is the administration of genes that will invoke the antitumor responses of the immune system.
- Adoptive immunotherapy. Active immunotherapy is the administration of genetically altered lymphocytes that are programmed to cause tumor destruction.
Complementary and Alternative Medicine
Many patients seek a more holistic or nontraditional approach, turning to complementary and alternative therapies while continuing to utilize conventional medicine.
- Complementary and Alternative Medicine (CAM). CAM was defined as diverse medical and health care systems, practices, and products that are not presently considered to be part of conventional medicine.
- Risk. Because of the possibility of herb-vitamin-drug interactions, there is concern about the use of biologicals and dietary supplements, which are not regulated by the FDA nor subjected to rigorous scientific evaluation.
Unproven and Unconventional Therapies
Hopelessness, desperation, unmet needs, lack of factual information, and family and social pressures are major factors that motivate patients to seek unconventional methods of treatment.
- Definition. Unconventional treatments are those without scientific evidence of the ability to cure or control cancer.
Nursing Management in Unconventional Therapies
The most effective way to protect patients and families from fraudulent therapies and questionable cancer cures is to establish a trusting relationship, provide supportive care, and promote hope.
- Communication. Truthful responses given in a nonjudgmental manner to questions and inquiries about unproven methods of cancer treatments may alleviate the fear and guilt on the part of the patient and the family that they are not “doing everything we can” to obtain a cure.
- Information. The nurse should inform the patient and family should inform the patient and family of the characteristics common to fraudulent therapies so that they will be informed and cautious when evaluating other forms of “therapy”.
- Collaboration. The nurse should encourage the patient to inform their physicians about the use of therapies to help prevent interactions with medications and other therapies that may be prescribed.
Nursing Care of Patients with Cancer
Main Article: 13 Cancer Nursing Care Plans
The outlook for patients with cancer has greatly improved because of scientific and technologic advances.
Maintaining Tissue Integrity
- Stomatitis. Assessment of the patient’s subjective experience and an objective assessment of the oropharyngeal tissues and teeth are important and for the treatment of oral mucositis, Palifermin (Kepivance), a synthetic form of human keratinocyte growth factor, could be administered.
- Radiation-associated skin impairment. Nursing care for patients with impaired skin reactions includes maintaining skin integrity, cleansing the skin, promoting comfort, reducing pain, preventing additional trauma, and preventing and managing infection.
- Alopecia. Nurses provide information about hair loss and support the patient and family in coping with changes in body image.
- Malignant skin lesions. Nursing care includes cleansing the skin, reducing superficial bacteria, controlling bleeding, reducing odor, protecting the skin from further trauma, and relieving pain.
Promoting Nutrition
- Anorexia. Anorexia may occur because people feel full after eating only a small amount of food.
- Malabsorption. Surgical intervention may change peristaltic patterns, later gastrointestinal secretions, and reduce the absorptive surfaces of the gastrointestinal mucosa, all leading to malabsorption.
- Cachexia. Nurses assess patients who are at risk of altered nutritional intake so that appropriate measures may be instituted prior to nutritional decline.
Relieving Pain
- Assessment. The nurse assesses the patient for the source and site of pain as well as those factors that increase the patient’s perception of pain.
- Cancer pain algorithm. Various opioid and nonopioid medications may be combined with other medications to control pain as adapted from the World Health Organization three-step ladder approach.
- Education. The nurse provides education and support to correct fears and misconceptions about opioid use.
Decreasing Fatigue
- Assessment. The nurse assesses physiologic and psychological stressors that can contribute to fatigue and uses several assessment tools such as a simple visual analog scale to assess levels of fatigue.
- Exercise. The role of exercise as a helpful intervention has been supported by several controlled trials.
- Pharmacologic interventions. Occasionally pharmacologic interventions are utilized, including antidepressants for patients with depression, anxiolytics for those with anxiety, hypnotics for patients with sleep disturbances, and psychostimulants for some patients with advanced cancer or fatigue that does not respond to any medication.
Improving Body Image and Self-esteem
- Assessment. The nurse identifies potential threats to the patient’s body image experience, and the nurse assesses the patient’s ability to cope with the many assaults to the body image experienced throughout the course of the disease and treatment.
- Sexuality. Nurses who identify physiologic, psychologic or communication difficulties related to sexuality or sexual function are in a key position to help patients seek further specialized evaluation and intervention if necessary.
Assisting in the Grieving Process
- Assessment. The nurse assesses the patient’s psychological and mental status, as well as the mood and emotional reaction to the results of diagnostic testing and prognosis.
- Grieving. Grieving is a normal response to these fears and to actual or potential losses.
Monitoring and Managing Potential Complications
- Infection. The nurse monitors laboratory studies to detect any early changes in WBC counts.
- Septic shock. Neurologic assessments are carried out, fluid and electrolyte status is monitored, arterial blood gas values and pulse oximetry are monitored, and IV fluids, blood, and vasopressors are administered by the nurse.
- Bleeding and hemorrhage. The nurse may administer IL-11, which has been approved by the FDA to prevent severe thrombocytopenia, and additional medications may be prescribed to address bleeding due to disorders of coagulation.
Promoting Home and Community-Based Care
Nurses in the outpatient settings often have the responsibilities for patient teaching and for coordinating care in the home.
- Teaching patients self-care. Follow-up visits and telephone calls from the nurse assist in identifying problems and are often reassuring, increasing the patient’s and the family’s comfort in dealing with complex and new aspects of care.
- Continuing care. The responsibilities of the home care include assessing the home environment, suggesting modifications at home or in care to help the patient and the family address the patient’s physical needs.
Originally published by Iris Dawn Tabangcora RN
Distinctive tumors were first reported in scientific journals in 1775, and that was scrotal cancer directly associated with chimney sweeps. In 1761, cases of nasal cancer rose among individuals who use snuff or smokeless tobacco. Since then, cancer has made its identity known as the disease that plagues the unsuspecting society.
Cancer can occur anywhere in the body. When the body’s normal control mechanisms become defective, old cells do not die and new abnormal cells continue to proliferate. Consequently, these extra cells form tissue masses which deprive the normal and healthy cells of the nutrients necessary for growth and development.
However, since there is still no cure for cancer, the healthcare industry advocates for prevention and early detection. Screening tests are made to subject persons suspected to have cancer but still do not have the manifestations yet. If the results are highly suggestive, a biopsy is conducted to confirm the working diagnosis.
Mortality Hit Around the World
World Health Organization (WHO) reported that in 2012, there were 14 million new cases of cancer and 8.2 million cancer-related deaths. Sixty percent of these new cases are from Africa, Asia, and some parts of America. In the United States alone, it is estimated that for 2016, there will be 1.6 million new cases of cancer and cancer-related deaths would reach half a million.
Nurses as Cancer Insurgents
When facing cancer, nurses understand the importance of early detection and treatment. This guarantees a relatively higher chance of surviving the savage disease. The problem with cancer is that it only signals its existence when it is already severe. Unlike other diseases, it does not scream pain. Most of the time, before one becomes aware of its existence, cancer has made a map out of one’s body and has lodged itself in every corner.
Nurses have witnessed parents become childless and children become orphaned because of cancer. Therefore, it is important for nurses to spread awareness on cancer and how it can be prevented in the earliest time possible. Nurses should learn cancer screening test guidelines by heart as part of the commitment to saving lives.
Cancer Screening Test Guidelines
Here are the screening test guidelines for different types of cancer according to American Cancer Society and U.S. Preventive Task Force Services:
1. Breast Cancer
Seventy percent of women have no known predisposing factors to breast cancer but certain risk factors have been established. Risk factors include age 65 and above, two first-degree relatives diagnosed with breast cancer at an early age, high breast tissue density, and factors that affect circulating hormones like late menopause, long-term use of hormonal replacement therapy, and obesity.
Breast cancer screening includes mammography, clinical breast examination (CBE), and breast self-examination (BSE). It is important that patients understand what these examinations are all about, how they are performed, and their limitations.
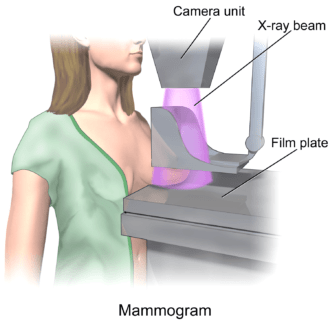
Mammography (x-ray of the breast) is done yearly for women age 40 and above. However, for women with increased risk, it may be started at age 30. CBE is done every 2-3 years among women 20-39 years of age and then annually after 40 years of age. Basically, this is a physical exam done by a healthcare provider as part of the regular medical check-up. Lastly, nurses should teach women 20 years of age and above on how to perform BSE. This should be done 5-7 days after menstruation when the breasts are not swollen and tender. For women with an irregular sexual cycle, a specific date must be chosen for monthly BSE.
2. Cervical Cancer
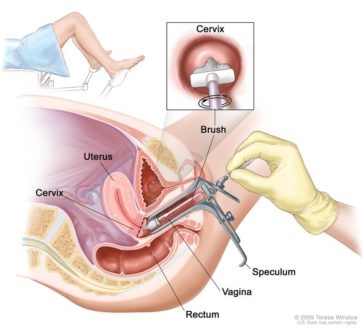
The screening test for cervical cancer is Pap Smear. In 2012, the American College of Obstetricians and Gynecologists (ACOG) released a new guideline for this test. First screening should be at age 21. For women age 21 to 39, screening is done every three years. Until age 60, screening is done with cytology if Pap Smear is positive or if the patient is at high-risk for HPV test. For women who have undergone hysterectomy for benign reasons, routine screening is discontinued. Lastly, for women age 65 and above, routine screening is discontinued if three consecutive Pap smear result is negative.
3. Ovarian Cancer
Currently, there is no effective screening test for ovarian cancer although risk factors would include history of breast or ovarian cancer in the family and mutation in BRCA1 and BRCA2 genes.
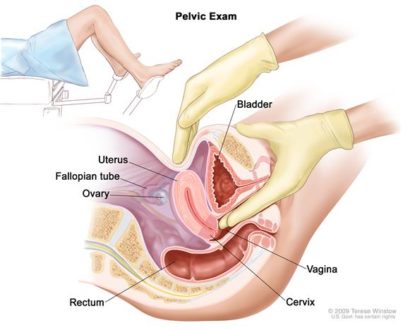
Pelvic exam is done upon check-up and the doctor would request ultrasound and magnetic resonance imaging (MRI) as needed.
4. Testicular Cancer
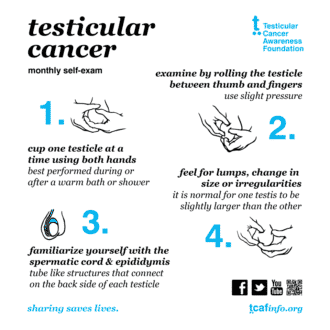
Monthly testicular self-examination (TSE) is recommended for men. A painless nodule or lump felt is always advised to be reported to the doctor. TSE should be done after a warm shower so the skin is relaxed.
5. Lung Cancer
Low-dose computer tomography annual screening for lung cancer is recommended for adults age 55-80 years with smoking history of 30 pack years or have quit smoking within 15 years. Screening is discontinued if the person has stopped smoking for at least 15 years.
6. Liver Cancer
American Cancer Society has no current recommendations for liver cancer screening. However, two most commonly requested test for liver cancer includes ultrasound and alpha-fetoprotein (AFP) blood test.
7. Colorectal Cancer
Screening recommendations for colorectal cancer include fecal occult blood test (FOBT), sigmoidoscopy, and colonoscopy.
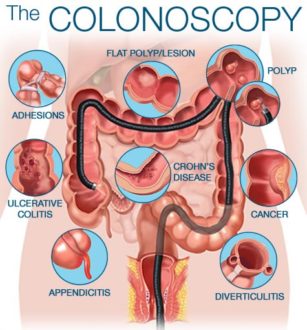
Assessment for risk factors (e.g. polyps, first-degree relative with colorectal cancer, personal history of ulcerative colitis, etc.) should begin at age 20. However, for those who are not high risk, routine screening recommendations should take place between 50 and 75 years of age.
FOBT is conducted annually. Another option is to have sigmoidoscopy every five years and FOBT every three years. Third option on the list is to have colonoscopy every 10 years.
8. Prostate Cancer
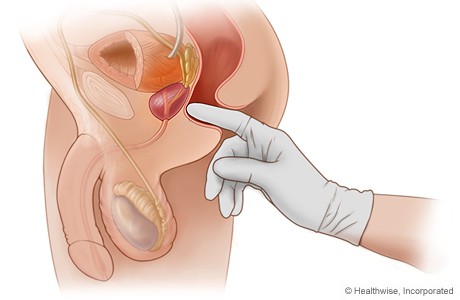
Prostate cancer is the leading cancer among men in the U.S. and the second leading cause of death. Risk factors include age, history of prostate cancer in the family and African American ethnicity. Screening recommendations include digital rectal examination (DRE) and prostate-specific antigen (PSA). However, these two methods are not highly accurate. DRE can miss as much as 25-35% of tumors and its sensitivity is only 59%. PSA’s detection rate is only 28-35%. It is being recommended to combine the two screening options for men above 50 years of age. For men with risk factors, screening should be started at age 40.
9. Skin Cancer
As of now, there’s not enough evidence to recommend a routine screening that can detect skin cancers early. However, it is important to note that fair-skinned individuals aged 65 and older are at increased risk for melanoma. Having atypical moles and/or more than 50 moles increase the risk of the person for melanoma too.
Pass The Word
How can you help stop cancer from taking away people’s lives? Take these screening guidelines to heart and spread awareness about early detection of different kinds of cancer.

























Leave a Comment