
Have you ever wondered what nurses do during the historic times? When mechanical ventilators are not yet invented, how do nurses manage to survive? Rather, did their patients back then survive?
Charles Darwin once said, “It is not the strongest of the species that survive, nor the most intelligent, but the one most responsive to change.”
Pondering upon this quote, we realize that the nursing profession survived because of our ability to adapt to changes. It is dynamic. Whatever innovation in nursing techniques we have not is because of how we embraced the evolution of healthcare.
Nightingale said: “Unless we are making progress in our nursing every year, every month, every week, take my word for it, we are going back.”
The past is important to move forward. And yes, we are entering a new era of nursing interventions.
Let’s hop in a time machine and travel back in time and learn about the practices we don’t do (hopefully for good) anymore.
1. Rotating tourniquets
Also known as congesting cuffs, are often used to treat patients with acute pulmonary edema secondary to heart failure during the 1960s. The idea was to pool the blood in the veins and decrease the venous return therefore ultimately decreasing pulmonary congestion. Congesting cuffs were placed on three extremities and inflated to 20 to 80 mmHg to achieve its effect.
Why did it disappear? Aside from being time-consuming, potent drugs like diuretics are available today. Studies also cannot support the effectivity of this practice.
2. Use of the artificial lung: “The Iron Lung Machine.”
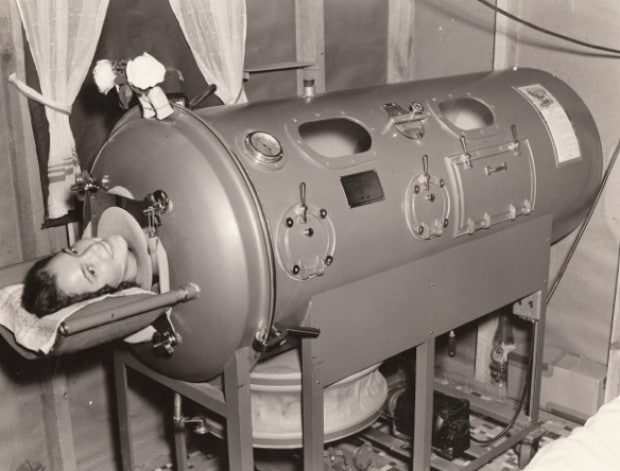
According to Wikipedia, the first of these devices to be widely used was developed by Drinker and Shaw in 1928. The iron lung often referred to in the early days as the “Drinker respirator,” was invented by Philip Drinker (1894–1972) and Louis Agassiz Shaw, Jr., professors of industrial hygiene at the Harvard School of Public Health.

Some of the Iron Lung machines are still used in the US, but only a few extinct nurses know how to use them.
Why did it disappear? The use of modern treatment and portable ventilators including the eradication campaign against polio – the last case of naturally occurring polio happened in 1979 – sparked the decline of the iron lung machine.
3. Reuse of urinary catheters and syringes
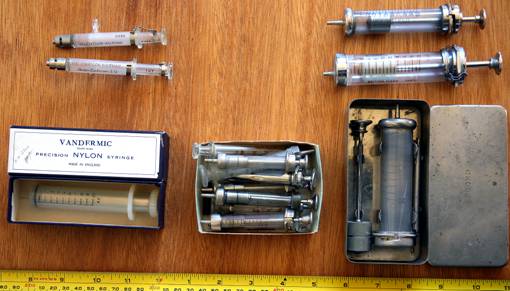
Back then, resterilization of syringes and urinary catheters were a trend. Syringes were made of glass and catheters were made of metal instead of the silicone we use today. Since they’re made of hardened materials, they were heat sterilized and immersed in alcohol– a practice that would be frowned upon today. Needles were not for single use and had to be sharpened manually. Yikes.
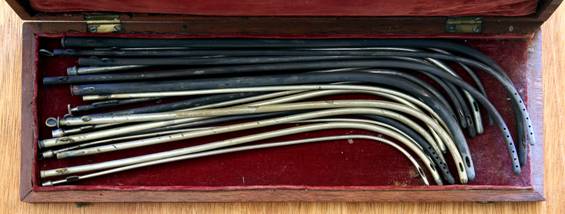
Why did it disappear? Single-use disposable syringes are the standard today ever since the occurrence of HIV and blood-borne pathogens. Different reusable equipment was produced because it’s safer and prevents cross contamination. Also, resterilizing is more costly for hospitals.
4. Notable antiseptic: Dakin’s Solution for wounds
Dakin’s solution was used mostly during the Worlds War I. It is composed of sodium hypochlorite and baking soda, and invented by a chemist and a surgeon. After the war, it was widely used for bedsores and infected wounds.

Why did it disappear? It didn’t! Some institutions still use this today though others prefer proven antiseptics like povidone iodine, etc.
5. Penthrane and Trilene inhalers for labor pain
An inhaler for pain relief was once introduced for pregnant women who can’t tolerate labor pain.

Trichloroethylene (Trilene) and methoxyflurane (Penthrane) were popular analgesics used in obstetrics during the 1900s. These were administered via a calibrated, temperature-compensated vaporizers given to a mother for PRN pain relief during labor.
Why did it disappear? The drugs were effective for pain relief, so effective that they caused maternal sedation as well as neonatal depression. It also caused vomiting and accumulation causing renal damage. Due to its adverse effects, its use was discontinued.
6. Sliding scale insulin with urine dipstick results
Before the dawn of the great glucometer, nurses have to obtain a patient’s urine sample before meals to test for the presence of glucose.
Why did it disappear? Usage of the urine dipstick test was not longer recommended as glucometer devices provide a more accurate measurement of a patient’s glucose levels.
7. Antacid to pressure ulcers
A retired senior nurse recalled applying an antacid to pressure ulcer believing it would heal the wound faster.
Why did it disappear? It is now well known that moist wound healing is the ideal environment for faster healing, according to various studies.
8. Controlling foul wound odor with charcoal
Back then nurses used to dab teaspoons charcoal and wrap gauze around an infected open wound to facilitate faster healing and to minimize the foul odor – thinking charcoal would absorb the odor.

Why did it disappear? It didn’t. Actually, some people still use activated charcoal for wounds thought the risk of infection is high in some instances.
9. Instilling saline solution to rinse mucus during suctioning.
It was then thought that saline acts as a lubricant in facilitating the ease of passage of the suction catheter with the same concept, it was also thought to loosen and dilute secretions and enhance a cough.

Why did it disappear? Instilling was often traumatic for patients, and cough reflex was not always elicited especially for people with tetraplegia with little or no diaphragm innervation. Prevalence of mucolytics to enhance mobilization of secretions is most commonly used. Studies have also proved that the practice increases the patient’s risk for pneumonia and the possibility of pushing bacterial formation deeper into the lungs.
10. Cut the Foley catheter before removal.
An old-school practice that deserves to stay as it is. The practice involves snipping an inserted indwelling foley catheter to facilitate easy removal.
Why did it disappear? The practice can be considered dangerous because the tension can cause the end left with the patient to retract into the bladder.
11. Milking chest tube drains
This involves squeezing, twisting, or kneading the chest tube to create bursts of suction to move clots and remove any visible secretions.
Why did it disappear? The reason is the risk of air leakage within the chest tube, which can cause irritation and tissue trauma around the insertion site of the tubing.
12. Coca-Cola to unclog nasogastric tubes.
Coca-cola (or any carbonated soda) is a notorious unclogger for feeding tubes. The acidity in cola is believed to help unclog the tube.
Why did it disappear? Coke, being an acidic fluid, can damage the integrity of the NG tube. It can also contribute to clogging by denaturing proteins in some enteral formulas. Water or replacing the tube is recommended.
Knowing these interventions is a revelation for present nurses. Nevertheless, these practices taught us a lesson: to continually improve and render the best and proven care we could give to our patients.
























Leave a Comment