Scoliosis is a musculoskeletal disorder that affects the spine, causing lateral curvature and rotation of the vertebral column. This common condition can manifest during childhood or adolescence, and in some cases, it may develop in adulthood due to various underlying factors. As nurses, our commitment to patient care extends beyond physical health, encompassing emotional support, education, and empowerment throughout the journey of managing scoliosis.
This article seeks to provide a comprehensive nursing perspective on scoliosis management, encompassing the early detection, assessment, and treatment of this condition.
What is Scoliosis?
The term scoliosis is derived from the Greek word skolios (“twisted”) and refers to a sideward (right or left) curve in the spine.
- Scoliosis is a condition that causes the spine to curve sideways in an “S” or “C” shape. It can affect people of all ages, but it is most commonly diagnosed during adolescence. Mild cases may not cause any symptoms, while severe scoliosis can lead to back pain, difficulty breathing, and changes in posture.
- Scoliosis is not a simple curve to one side but, in fact, is a more complex three-dimensional deformity that often develops in childhood.
- The term infantile scoliosis is used specifically to describe scoliosis that occurs in children younger than 3 years.
- Other terms for scoliosis also depend on the age of onset, such as juvenile scoliosis (4-9 years) and adolescent scoliosis (10-18 years).
- Scoliosis is a lateral curvature of the spine, that occurs in two forms: structural and functional (postural).
Types
There are two types of scoliosis:
- Structural. Structural scoliosis involves rotated and malformed vertebrae.
- Functional. Functional scoliosis, the more common type, can have several causes: poor posture, muscle spasms caused by trauma, or unequal length of legs.
Pathophysiology
Most cases of structural scoliosis are idiopathic; a few are caused by congenital deformities or infections.
- Most of the curves in the spine develop during the first year of life, and a strong correlation has been found between the nursing posture of the infant and the development of the curve.
- It is less common in the United States than in Europe, where babies are nursed in the supine position.
- Infants have a natural tendency to turn toward the right side, and because of the plasticity of the infant’s axial skeleton, this can lead to the development of plagiocephaly, bat ear on the right side, and curvature of the spine toward the left side.
Statistics and Incidences
Many states require regular examination of students for scoliosis, beginning in the fifth or sixth grade.
- Scoliosis is a rare condition, accounting for fewer than 1% of cases of idiopathic scoliosis in North America; in Europe, the rate is 4%.
- Males account for 60% of the cases of early-onset scoliosis; 90% of the cases of early-onset scoliosis resolve spontaneously, but the other 10% progress to a severe and disabling condition.
- Females constitute 90% of late-onset cases and need close monitoring to allow intervention at appropriate times.
- Idiopathic scoliosis is seen in school-age children at 10 years of age and older.
- Although mild curves occur as often in boys as in girls, idiopathic scoliosis requiring treatment occurs eight times more frequently in girls than in boys.
Causes
Although the exact cause of scoliosis is not known, hypotheses have been proposed on the basis of epidemiologic evidence.
- Mechanical factors. One theory holds that the mechanical factors during intrauterine life are responsible for the higher incidence of plagiocephaly, developmental dysplasia of the hip, and scoliosis on the same side of the body.
- Genetic and external factors. A second hypothesis suggests multifactorial causes, including predisposing genetic factors that are either facilitated or inhibited by external factors such as defective motor development or collagen disorders, joint laxity, and nursing posture of the infant.
- Other factors. Other associations include older mothers from poorer families, breech presentation, and premature and male low-birth-weight babies.
Clinical Manifestations
Infantile scoliosis usually is detected during the first year of life either by the parents or by the pediatrician during a routine examination of the infant.
- Thoracic curve. Usually, a single long thoracic curve to the left is present; less often, a thoracic and lumbar double curve is noted.
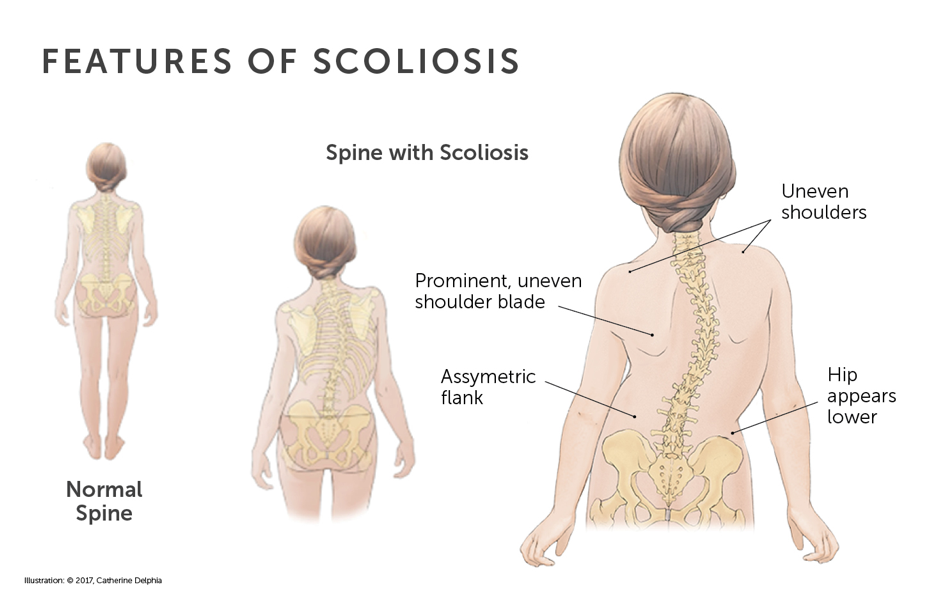
- Asymmetry. Observe asymmetry of the shoulders, shoulder blades, or hips.
- Unequal distance of extremities. There is an unequal distance between the arms and waist.
Assessment and Diagnostic Findings
Diagnosis is made based on screening examination.
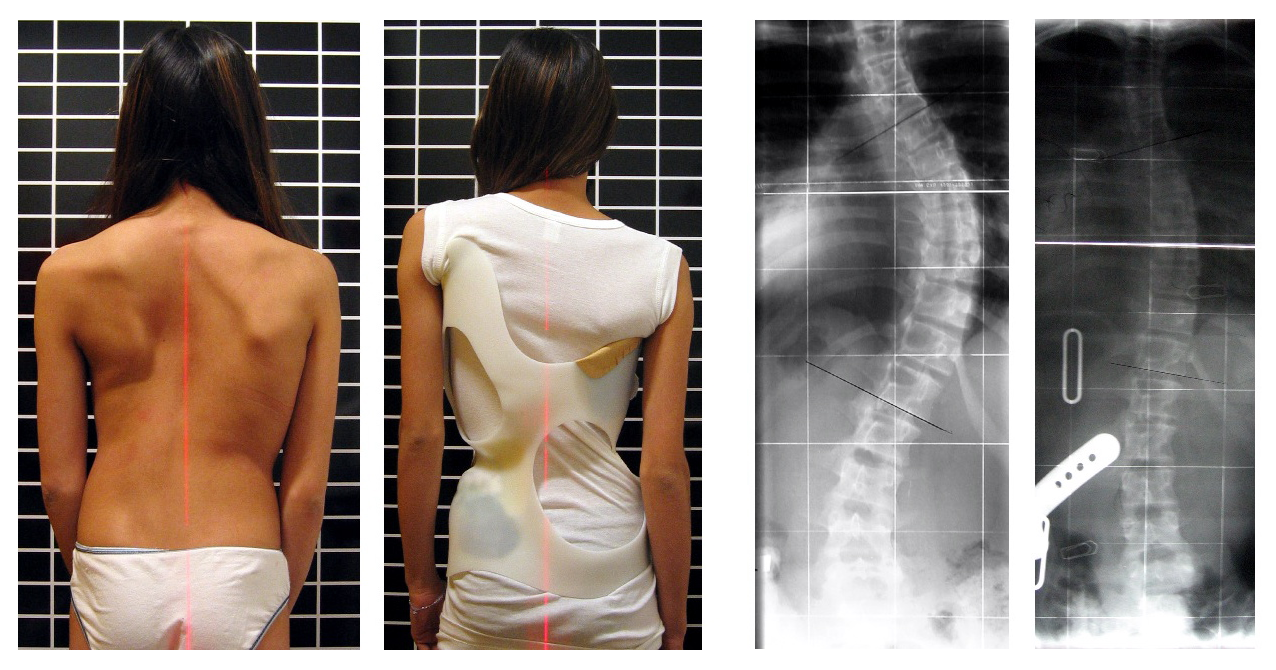
- Radiography. Radiographs of the spine in infants are taken with the child held up by the arms; the severity of the scoliosis is established by calculating the rib-vertebral angle difference (RVAD) in the radiographs.
- Computed tomography (CT). Computed tomography can be used to get a detailed picture of the scoliosis curve.
- Magnetic resonance imaging (MRI). Magnetic resonance imaging is necessary in moderate-to-severe scoliosis because the reported frequency of neural axis abnormalities associated with scoliosis has been high (21-50% in some sources).
Medical Management
Treatment depends on many factors and is either surgical or non-surgical.
Nonsurgical Management
Treatment is long-term and often lasts through the rest of the child’s growth cycle.
- Electrical stimulation. Electrical stimulation may be used as an alternative to bracing for a child with a mild to moderate curvature; treatment occurs at night when the child is asleep, electrodes are applied to the skin; the leads are placed to stimulate muscles on the convex side of the curvature to contract as impulses are transmitted; this cause the spine to straighten.
- Braces. The Boston brace or the TLSO brace is more commonly used to treat scoliosis; the brace should be worn constantly, except during bathing and swimming; its fit is monitored closely; it is worn over a T-shirt or undershirt to protect the skin.
- Pedicle screw instrumentation. Because of advances in instrumentation, pedicle screw instrumentation can be performed for children with further growth potential; in these patients, a growing rod is used, which is associated with fewer complications than surgical fixation using L-rods.
- Halo traction. When a child has a severe spinal curvature or cervical instability, a form of traction known as halo traction may be used to reduce spinal curves and straighten the spine.
Surgical Management
The decision of whether to operate on a patient with scoliosis depends on many factors.
- Growing rods. Growing rods without fusion is preferable until combined posterior and anterior fusion can be done; growing-rod systems (eg, pediatric Isola instrumentation) may be utilized to prevent curve progression; extensions are needed every 6 months to keep pace with the child’s growth until the child has adequate trunk length, which is usually between the ages of 11 and 15 years.
- Localizer cast. A localizer cast can hold the curve and prevent it from progressing further; the localizer cast is applied to the child’s trunk under general anesthesia, with traction to the head and neck via a sling across the mandible and the occiput and countertraction to the pelvis through another sling; the plaster jacket is applied around the trunk, with care taken to ensure that there is enough room for hip movements by stopping just below the level of the iliac wings; superiorly, the plaster goes around the axillae, leaving the arms and the shoulders free.
- Pediatric Isola spine system. The Isola system consists of screws with washers that are applied from posterior to anterior, horizontal to the frontal plane of the vertebral body, and parallel to the apex of the curvature.; screws may be applied through the staples; rods are inserted to prevent progression of the curve, and the rods are extended every 6 months to keep pace with the child’s growth.
Nursing Management
Nurses play an important role in the management of a child with scoliosis, especially for postoperative care.
Nursing Assessment
A child with scoliosis must be reassessed every 4 to 6 months.
- Degree of curvature. Document the degree of curvature and related impairments.
- Provide privacy. Provide privacy and protect the child’s modesty.
- Assess emotional status. Be sensitive to the emotional state of the child; the family caregivers also may be upset but try to hide it for the child’s sake.
Nursing Diagnoses
Based on the assessment data, the major nursing diagnoses are:
- Impaired physical mobility related to restricted movement.
- Risk for injury related to decreased mobility.
- Risk for impaired skin integrity related to irritation of brace.
- Risk for disturbed body image related to wearing a brace continuously.
- Risk for noncompliance related to long-term treatment.
Nursing Care Planning and Goals
Main Article: 4 Scoliosis Nursing Care Plans
Major nursing care planning goals for a child with scoliosis include:
- Minimizing the disruption of activities.
- Preventing injury.
- Maintaining skin integrity and self-image.
- Complying with long-term care.
Nursing Interventions
Nursing interventions appropriate for a child with scoliosis are:
- Promote mobility. Prescribed exercises must be practiced and performed as directed; this can help to minimize the risks of immobility and promote self-esteem.
- Prevent injury. Evaluate the child’s environment after the brace has been applied and take precautions to prevent injury; help the child practice moving about safely; advise the family caregiver to contact school personnel to ensure that the child has comfortable, supportive seating at school.
- Prevent skin irritation. Check the child regularly to confirm the proper fit of the brace; observe for any areas of rubbing, discomfort, or skin irritation and adjust the brace as necessary; skin under the pads should be massaged daily; and daily bathing is essential.
- Promote positive body image. The child should be involved in all aspects of care planning; it is important for the child to have an opportunity to talk about his or her feelings; help the child select clothing that blends with current styles but is loose enough to hide the brace.
- Promote compliance with therapy. The child must wear the brace for years until spinal growth is completed; during this period, the caregivers and the child need emotional support from healthcare personnel; to encourage compliance, and teach them about possible complications of spinal instability and possible further deformity if correction is unsuccessful.
Evaluation
Goals are met as evidenced by:
- Minimized disruption of activities.
- Prevention of injury.
- Maintained skin integrity and self-image.
- Compliance with long-term care.
Documentation Guidelines
Documentation for a child with scoliosis includes:
- Individual findings include factors affecting, interactions, the nature of social exchanges, and specifics of individual behavior.
- Cultural and religious beliefs, and expectations.
- Plan of care.
- Teaching plan.
- Responses to interventions, teaching, and actions performed.
- Attainment or progress toward the desired outcome.


























Leave a Comment