
Hirschsprung disease is a congenital condition that affects the large intestine, resulting in a lack of nerve cells in certain segments of the bowel. This absence of nerve cells leads to a functional obstruction, causing difficulties in passing stool and potential complications like constipation and abdominal distension. Hirschsprung disease is typically diagnosed in infancy or early childhood, and prompt recognition and intervention are vital to prevent severe complications.
This nursing note provides an overview of Hirschsprung disease, discussing its etiology, clinical manifestations, diagnostic approaches, medical management, and nursing interventions.
What is Hirschsprung Disease?
In some cases, aganglionic megacolon or Hirschsprung disease may be severe enough to be recognized.
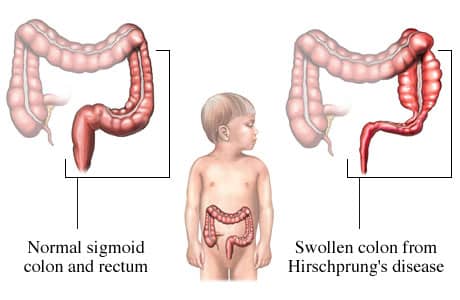
- Congenital aganglionic megacolon, also called Hirschsprung disease, is characterized by persistent constipation resulting from partial or complete intestinal obstruction of mechanical origin.
- In 1886, Harold Hirschsprung first described Hirschsprung’s disease as a cause of constipation in early infancy.
- Early recognition and surgical correction of Hirschsprung disease protect affected infants from enterocolitis and debilitating constipation.
Pathophysiology
The pathophysiology of aganglionic megacolon is as follows:
- Hirschsprung disease results from the absence of enteric neurons within the myenteric and submucosal plexus of the rectum and/or colon.
- Enteric neurons are derived from the neural crest and migrate caudally with the vagal nerve fibers along the intestine.
- These ganglion cells arrive in the proximal colon by 8 weeks gestation and in the rectum by 12 weeks gestation.
- Arrest in migration leads to an aganglionic segment.
- This results in clinical Hirschsprung disease.
Statistics and Incidences
Cases of aganglionic megacolon are seen in approximately 1 per 5000 live births.
- Prevalence may vary by region and has been shown to be as high as 1 per 3000 live births in the Federated States of Micronesia.
- The overall mortality of Hirschsprung enterocolitis is 25-30%, which accounts for almost all of the mortality from Hirschsprung disease.
- Hirschsprung disease is approximately 4 times more common in males than females.
- Nearly all children with Hirschsprung disease are diagnosed during the first 2 years of life.
- Approximately one-half of children affected with this disease are diagnosed before they are aged 1 year; a small number of children with Hirschsprung disease are not recognized until much later in childhood or adulthood.
Causes
The causes of aganglionic megacolon are:
- Genetic causes. The disease is generally sporadic, although the incidence of familial disease has been increasing; multiple loci appear to be involved, including chromosomes 13q22, 21q22, and 10q; mutations in the Ret proto-oncogene have been associated with multiple endocrine neoplasias (MEN) 2A or MEN 2B and familial Hirschsprung disease; other genes associated with Hirschsprung disease include the glial cell-derived neurotrophic factor gene, the endothelin-B receptor gene, and the endothelin-3 gene.
- Associated conditions. Hirschsprung disease is strongly associated with Down syndrome; 5-15% of patients with Hirschsprung disease also have trisomy 21; other associations include Waardenburg syndrome, congenital deafness, malrotation, gastric diverticulum, and intestinal atresia.
Clinical Manifestations
Examination of infants affected with Hirschsprung disease reveals:
- Abdominal distention. Infants with aganglionic megacolon show tympanitic abdominal distention and symptoms of intestinal obstruction.
- Chronic constipation. Older infants and children with Hirschsprung disease usually present with chronic constipation.
- Palpable intestinal loops. Upon abdominal examination, these children may demonstrate marked abdominal distention with palpable dilated loops of the colon.
- Absence/delayed passage of meconium. During the newborn period, infants affected with Hirschsprung disease may present with failure of passage of meconium.
- Vomiting. Repeated vomiting is present due to intestinal obstruction.
- Malnourishment. Poor nutrition results from the early satiety, abdominal discomfort, and distention associated with chronic constipation.
Assessment and Diagnostic Findings
The diagnosis of aganglionic megacolon is made through the following data:
- Laboratory studies. CBC count, order this test if enterocolitis is suspected; elevation of WBC count or a bandemia should raise concern for enterocolitis.
- Plain abdominal radiography. Perform this test with any signs or symptoms of abdominal obstruction.
- Unprepared single-contrast barium enema. If perforation and enterocolitis are not suspected, an unprepared single-contrast barium enema may help establish the diagnosis by identifying a transition zone between a narrowed aganglionic segment and a dilated and normally innervated segment; the study may also reveal a non distensible rectum, which is a classic sign of Hirschsprung disease.
- Rectal biopsy. Diagnosis is confirmed through rectal biopsy.
- Rectal manometry. In older children who present with chronic constipation and an atypical history for either Hirschsprung disease or functional constipation, anorectal manometry can be helpful in making or excluding the diagnosis.
Medical Management
Treatment involves:
- Initial therapy. If a child with Hirschsprung disease has symptoms and signs of a high-grade intestinal obstruction, initial therapy should include intravenous hydration, withholding of enteral intake, and intestinal and gastric decompression.
- Decompression. Decompression can be accomplished through the placement of a nasogastric tube and either digital rectal examination or normal saline rectal irrigations 3-4 times daily.
- Diet. A special diet is not required; however, preoperatively and in the early postoperative period, infants on a nonconstipated regimen, such as breast milk, are more easily managed.
Pharmacologic Management
Drug therapy currently is not a component of the standard of care for this disease itself; however, some medications may be used to treat complications of Hirschsprung disease.
- Antibiotics. Administer broad-spectrum antibiotics to patients with enterocolitis.
Surgical Management
The surgical options vary according to the patient’s age, mental status, ability to perform activities of daily living, length of the aganglionic segment, degree of colonic dilation, and presence of enterocolitis.
- Leveling colostomy. Surgical options include leveling colostomy, which is a colostomy at the level of normal bowel; a staged procedure with placement of a leveled colostomy followed by a pull-through procedure.
- Single-stage pull-through procedure. The single-stage pull-through procedure may be performed with laparoscopic, open, or transanal techniques; this procedure can be performed at the time of diagnosis or after the newborn has had rectal irrigations at home and has passed the physiologic nadir.
Nursing Management
Nursing care management for a child with aganglionic megacolon includes:
Nursing Assessment
Assessment involves:
- History. Carefully gather history from the family caregivers, noting especially the history of stooling; ask about the onset of constipation, the character and odor of stools, the frequency of bowel movements, and the presence of poor feeding habits, anorexia, and irritability.
- Physical examination. During the physical exam, observe for distended abdomen and signs of poor nutrition; record weight and vital signs.
Nursing Diagnosis
Based on the assessment data, the major nursing diagnoses for Hirschsprung disease are:
- Constipation related to decreased bowel motility.
- Imbalanced nutrition: less than body requirements related to anorexia.
- Fear (in the older child) related to impending surgery.
- Risk for impaired skin integrity related to irritation from the colostomy.
- Acute pain related to the surgical procedure.
- Deficient fluid volume related to postoperative condition.
- Impaired oral and nasal mucous membranes related to NPO status and irritation from NG tube.
- Deficient knowledge of caregivers related to understanding of postoperative care of the colostomy.
Nursing Care Planning and Goals
The major nursing care planning goals for patients with Hirschsprung Disease are:
- Maintaining skin integrity.
- Promoting comfort.
- Maintaining fluid balance.
- Maintaning moist, clean nasal and oral membranes.
- Reducing caregiver anxiety.
Nursing Interventions
Nursing interventions for a child with aganglionic megacolon include:
- Promote skin integrity. When performing routine colostomy care. give careful attention to the area around the colostomy; record and report redness, irritation, and rashy appearances of the skin around the stoma; prepare the skin with skin-toughening preparations that strengthen it and provide better adhesion of the appliance.
- Promote comfort. Observe for signs of pain, such as crying, pulse, and respiration rate increases, restlessness, guarding of the abdomen, or drawing up the legs; administer analgesics as ordered; additional nursing measures that can be used are changing the child’s position, holding the child when possible, stroking, cuddling, and engaging in age-appropriate activities.
- Maintain fluid balance. Accurate intake and output determinations and reporting the character, amount, and consistency of stools help determine when the child may have oral feedings; to monitor fluid loss, record and report the drainage from the NG tube every 8 hours; and immediately report any unusual drainage, such as bright-red bleeding.
- Provide oral and nasal care. Perform good mouth care at least every 4 hours; at the same time, gently clean the nares to relieve any irritation from the NG tube.
- Provide family teaching. Show the family caregiver how to care for the colostomy at home; discuss topics such as devices and their use, daily irrigation, and skin care; the caregivers should demonstrate their understanding by caring for the colostomy under the supervision of nursing personnel several days before discharge.
Evaluation
Goals are met as evidenced by:
- The child’s skin integrity is maintained.
- The child’s behavior indicates minimal pain.
- The child’s fluid intake is adequate.
- The child’s oral and nasal mucous membranes remain intact.
- The family caregivers demonstrated skill and knowledge in caring for the colostomy.
Documentation
Documentation in a patient with aganglionic megacolon includes:
- Individual findings include factors affecting, interactions, the nature of social exchanges, and specifics of individual behavior.
- Intake and output.
- Signs of infection.
- Cultural and religious beliefs, and expectations.
- Plan of care.
- Teaching plan.
- Responses to interventions, teaching, and actions performed.
- Attainment or progress toward the desired outcome.
























Leave a Comment