Respiratory Syncytial Virus (RSV) is a common and highly contagious viral infection that affects the respiratory system, causing symptoms ranging from mild cold-like symptoms to severe lower respiratory tract infections, particularly in infants and young children.
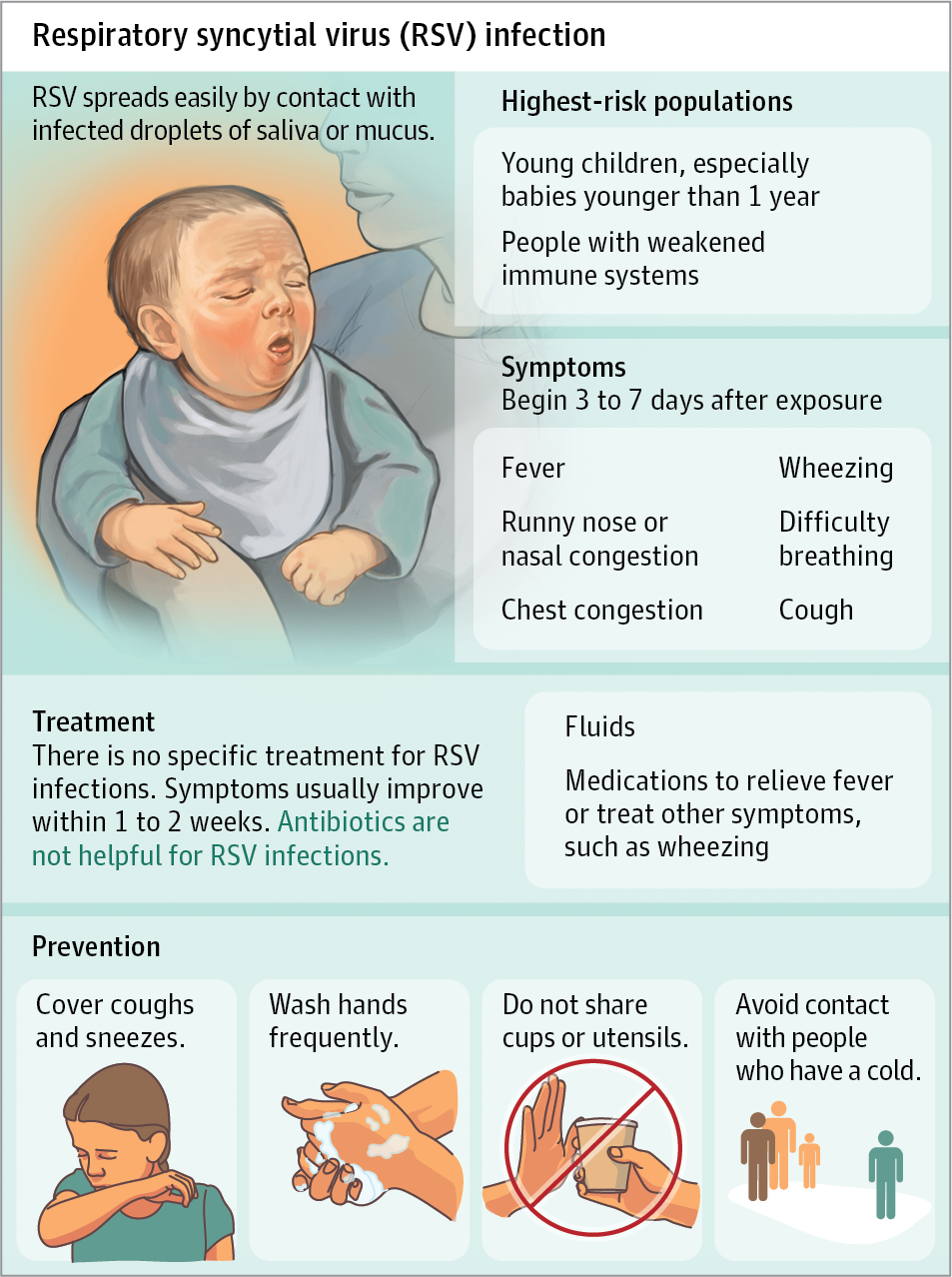
This contagious virus spreads through respiratory droplets, making early recognition, infection control measures, and supportive care needed in preventing further transmission.
What is Respiratory Syncytial Virus?
- Infection with respiratory syncytial virus which manifests primarily as bronchiolitis or viral pneumonia, is the leading cause of lower respiratory tract infections (LRTIs) in infants and young children.
- RSV can cause severe infection in some people, especially premature babies, older adults, infants and adults with heart and lung disease, or anyone with a very weak immune system (immunocompromised).
- Subsequently, RSV has been associated with bronchiolitis and LRTI in infants.
Pathophysiology
RSV infection is limited to the respiratory tract.
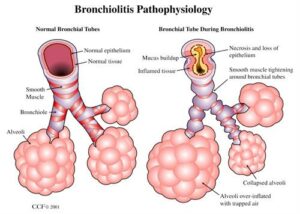
- Initial infection in young infants or children frequently involves the lower respiratory tract and most often manifests as the clinical entity of bronchiolitis.
- Inoculation of the virus occurs in the respiratory epithelial cells of the upper respiratory tract.
- Spread of the virus down the respiratory tract occurs through cell-to-cell transfer of the virus along intracytoplasmic bridges (syncytia) from the upper to the lower respiratory tract.
- The illness may begin with upper respiratory symptoms and progress rapidly over 1-2 days to the development of diffuse small airway disease characterized by cough, coryza, wheezing and rales, low-grade fever (< 101°F), and decreased oral intake.
Statistics and Incidences
Multiple epidemiologic studies have confirmed the role of this virus as the leading cause of LRTI in infants and young children.
- RSV LRT infection develops annually in 4-5 million children, and more than 125,000 children are admitted per year for RSV-related illness.
- Worldwide, RSV infection is prevalent, with clinical manifestations and early occurrence of RSV LRTI comparable to those seen in the United States.
- Severe RSV disease is primarily a disease of young infants and children, with a peak occurrence at the age of 2-8 months.
- Although boys and girls are equally affected by milder RSV disease, males are approximately twice as likely to be hospitalized for RSV disease.
- All races appear to be susceptible to RSV, showing similar disease patterns.
Causes
In the community setting, a number of factors have been associated with an increased risk of acquiring RSV disease, including the following:
- Childcare attendance. Children who attend childcare centers or who have siblings who attend school are at a higher risk of exposure.
- Lower socioeconomic status. People who have a low socioeconomic status tend to be at a higher risk for RSV.
- Prematurity. Prematurity, especially birth at less than 35 weeks gestation, makes the infant susceptible to RSV.
Clinical Manifestations
Patients with respiratory syncytial virus (RSV) infection may present with the following symptoms:
- Fever. A child experiences low-grade fever.
- Cough. Cough is also a common symptom of RSV.
- Tachypnea. There is an increase in the respiratory rate of the child.
- Retractions. The use of accessory muscles can be seen in children with RSV.
- Wheezing. There is audible wheezing upon auscultation.
Assessment and Diagnostic Findings
Specific diagnostic tests for confirmation of respiratory syncytial virus (RSV) infection are readily available.
- Culture tests. These tests can be performed on samples of secretions obtained by washing, suctioning, or swabbing the nasopharynx.
- Molecular probes. Molecular probes for revealing RSV in clinical specimens may be more sensitive than the aforementioned assays and are becoming clinically available, but they presently are more expensive.
- Antigen detection. The antigen detection methods offer the potential for diagnosis within hours and may be obtained reliably in the absence of a sophisticated virology laboratory.
- Chest radiography. Chest radiography is frequently obtained in children with severe RSV infection; typically, it reveals hyperinflated lung fields with a diffuse increase in interstitial markings.
Medical Management
Supportive care is the mainstay of therapy for respiratory syncytial virus (RSV) infection.
- Oxygen administration. Administration of supplemental oxygen guided by respiratory rates, work of breathing, oxygen saturation, and arterial blood gas values, as indicated is performed.
- Intravenous fluids. A brief course of intravenous (IV) fluids is generally administered in this setting, with the resumption of normal feeding as the child recovers (typically over 2-3 days).
- Fluid replacement. If the child can take in fluids by mouth and tolerate room air, outpatient management (with close physician contact as needed) is reasonable, especially in the absence of significant underlying risk factors.
Pharmacologic Management
At least a subset of patients with RSV-related lower respiratory tract infection (LRTI) appears to benefit from:
- Bronchodilators. Bronchodilator therapy with beta-agonists is frequently used, though data on the potential beneficial effects of such agents in this condition are conflicting.
- Antivirals. Ribavirin, a broad-spectrum antiviral agent in vitro, is licensed by the US Food and Drug Administration (FDA) for the aerosolized treatment of children with severe RSV disease.
Nursing Management
Nursing management for a child with RSV include:
Nursing Assessment
Assessment for a child with RSV includes:
- Vital signs. Assess the patient’s vital signs especially the respiratory rate and cardiac rate.
- History. Interview patient and caregivers regarding the medical history of the child.
- Physical examination. Note if there are any retractions and signs of severe respiratory distress.
Nursing Diagnoses
Based on the assessment data, the major nursing diagnoses are:
- Impaired gas exchange related to possible viral pneumonia.
- Fluid volume deficit related to decreased fluid intake.
- Hyperthermia related to dehydration.
Nursing Care Planning and Goals
The major nursing care planning goals for respiratory syncytial virus are:
- Patient will experience ease of breathing.
- Patient will not experience dyspnea at rest.
- Respiratory rate is within normal limits.
- Absence of fever.
Nursing Interventions
Nursing interventions for a child with RSV are:
- Use of humidified air. Keep the room warm but not overheated; if the air is dry, a cool-mist humidifier or vaporizer can moisten the air and help ease congestion and coughing; be sure to keep the humidifier clean to prevent the growth of bacteria and molds.
- Encourage oral fluid intake. Keep a steady supply of cool water at the bedside; offer warm fluids, such as soup, which may help loosen thickened secretions; ice pops may be soothing as well; continue breastfeeding or bottle-feeding your infant as you would normally.
- Encourage good hygiene habits. Teach your children the importance of hand-washing; use your own glass or disposable cups when you or someone else is sick; label each person’s cup.
- Administer medications. Give prescribed medications and encourage compliance.
Evaluation
Goals are met as evidenced by:
- Patient experienced ease of breathing.
- Patient experienced dyspnea at rest.
- Respiratory rate is within normal limits.
- Absence of fever.
Documentation Guidelines
Documentation in a child with RSV includes:
- Temperature and other assessment findings, including vital signs.
- Causative and contributing factors.
- Impact of condition on personal image and lifestyle.
- Plan of care.
- Teaching plan.
- Responses to interventions, teaching, and actions performed.
- Attainment or progress towards desired outcomes.
- Modifications to plan of care.


























Leave a Comment